After much thought and deliberation, and for various reasons both altruistic and sensible, I have decided to stop writing this blog. I feel that it has served it's purpose for me, and I have been delighted to share both misery and joy with a lot of like-minded anaesthetists.
It's not all bad news - I have now become the Final FRCA Resource Editor on AnaesthesiaUK. What I plan to do is help create a new, updated Final FRCA section on the website, using my experience and materials gained in writing this blog.
Many Thanks for all your support over the past year!
Best Wishes
James
Monday, 9 February 2009
Saturday, 20 December 2008
Wind-down
Thank you to all the messages you have all left. I hope those who passed are enjoying a bit of freedom. To those who weren't successful, I appreciate how you are feeling having been through it myself.
This time around, I managed to get 2's in all sections of the exam which I was really chuffed about (I seriously thought I was on a 1+ for the Science Viva!). Below is a summary of my exam:
Long Case
"The one with the malignant melanoma on her back" Straight from Mills, Maguire, & Barker Clinical Viva Book p.167.
-COPD (obstructuve PFTs, RLL pneumonia), HTN (mild renal failure, LVH/strain on ECG). On enalapril - still hypertensive.
-Preoptimisation, antihypertensives, pathophys of malignant melanoma (I said more common in gingers - they loved that!), prone position + complications. Anaesthesia. HDU/ICU
Short Cases
1) Obese man for knee arthroscopy, cardiac stent one year ago, only on statin and ACE-i. ECG Qwaves inf, TWi anterolat. Preoptimisation, stents, ?regional + NOT day case!
2) Dural Tap straight from Bricker SAQ book! What do you do? They steered me towards spinal catheter and it's management +doses + pathophysiology of PDPH.
3) 8yo boy RTA #tib/fib GCS 8/15. Straightforward airway management in trauma case. They placed a lot of emphasis on C-spine protection.
Science
Anatomy - 'Where can the phrenic nerve be damaged?'. Causes of damage + course of nerve.
Physiology - Renal replacement therapy in ICU including drawing of CVVHF/CVVHDF circuits + Rx of life-threatening hyperkalaemia.
Physics - Humidification - different methods. HME filters. Pathophysiology of damage to airways by not humidifying gases
Pharmacology - 'You have given 8mg vecuronium and at the end of a 1hr operation there is no response to peripheral nerve stimulation.' Discuss possibilities. Moved on discussion of NMJ. Don't forget simple things like machine failure.
Hope this helps.
This time around, I managed to get 2's in all sections of the exam which I was really chuffed about (I seriously thought I was on a 1+ for the Science Viva!). Below is a summary of my exam:
Long Case
"The one with the malignant melanoma on her back" Straight from Mills, Maguire, & Barker Clinical Viva Book p.167.
-COPD (obstructuve PFTs, RLL pneumonia), HTN (mild renal failure, LVH/strain on ECG). On enalapril - still hypertensive.
-Preoptimisation, antihypertensives, pathophys of malignant melanoma (I said more common in gingers - they loved that!), prone position + complications. Anaesthesia. HDU/ICU
Short Cases
1) Obese man for knee arthroscopy, cardiac stent one year ago, only on statin and ACE-i. ECG Qwaves inf, TWi anterolat. Preoptimisation, stents, ?regional + NOT day case!
2) Dural Tap straight from Bricker SAQ book! What do you do? They steered me towards spinal catheter and it's management +doses + pathophysiology of PDPH.
3) 8yo boy RTA #tib/fib GCS 8/15. Straightforward airway management in trauma case. They placed a lot of emphasis on C-spine protection.
Science
Anatomy - 'Where can the phrenic nerve be damaged?'. Causes of damage + course of nerve.
Physiology - Renal replacement therapy in ICU including drawing of CVVHF/CVVHDF circuits + Rx of life-threatening hyperkalaemia.
Physics - Humidification - different methods. HME filters. Pathophysiology of damage to airways by not humidifying gases
Pharmacology - 'You have given 8mg vecuronium and at the end of a 1hr operation there is no response to peripheral nerve stimulation.' Discuss possibilities. Moved on discussion of NMJ. Don't forget simple things like machine failure.
Hope this helps.
Tuesday, 9 December 2008
It's Good News!
After thirteen months, I have finally passed the Final FRCA. Many thanks to those who have helped me (you know who you are) and many thanks to those who have been so supportive of this blog both yesterday and in the last few months.
Best of luck to the guys and gals for the rest of the week!
Best of luck to the guys and gals for the rest of the week!
Sunday, 7 December 2008
All the best
Best of luck to everyone taking the exam this week - I'd like to think that if we've put the work in and done the viva practice, we deserve to pass this marathon!
Thanks to all who've left messages of support on this blog: nice to know that there are others sharing the pain.
Looking forward to a pint or two tomorrow afternoon in the Square Pig - come and find me, I'm easy to spot: tall with red hair!!
Thanks to all who've left messages of support on this blog: nice to know that there are others sharing the pain.
Looking forward to a pint or two tomorrow afternoon in the Square Pig - come and find me, I'm easy to spot: tall with red hair!!
Friday, 5 December 2008
X-Rays & CTs
Following a request for xrays/CTs etc, I have made available a Powerpoint file which I have put together with some films I have found/collected/used in the past. One film is taken after one of my clinical interventions (not telling you which one though!).
You can view the file from the website and can download it if you register (for free).
You can view the file from the website and can download it if you register (for free).
Sunday, 30 November 2008
Up and down and up and down
There is a reason for my infrequent postings at present - I'm trying desperately hard to pass this bloody exam! I've been seeking out viva practice where I can (word of note: don't tell the attractive ODP that you're looking for any consultants for oral examination practice!), practicing graphs, diagrams, and equations, and trying desperately to remember the cardiac cycle for the sixteenth time in my career at least.
It has been such a rollercoaster ride during viva practices. There are some sessions where I am concise, calm, and knowledgeable, then there are the ones where I have completely crumpled and been close to tears with frustration at having such a poor memory. Actually, there are a few words of advice I would like to impart, both from experience of preparation and the day itsself.
The next week
-Don't overdo it - you can't read whole textbooks in one day. Plan sensibly.
-Another piece of excellent advice I was given, is to imagine that the structure of your answer is analogous to a tree. Do not aim for the fruit immediately - start with the trunk (or DEFINITION) and a few main branches thereafter (CLASSIFY). The examiner will guide you towards which piece of fruit to pick and digest upon!!
-Learn to classify drugs. I use Sasada & Smith which breaks them up nicely into different categories.
-Always talk about drugs in terms of dose by weight e.g. 5mg/kg rather that 150mg (especially in paediatrics.
-Try not to A-Z chase - you know the sport. Open the A to Z and read a topic, then see a boldly outlined word so turn to that topic etc etc. You'll be there for ever.
-Make sure you can interpret and describe ECGs/CXR/basic CT etc.
-Refamiliarise yourself with some recent guidelines/topics. most have been mentioned previously in this blog.
-Have a look at the RCOA Finals Guide - just occaisionally some of the Short Cases/Long Cases/Basic Science stuff comes up word for word.
On the day
-Usual advice of arrive early, dress smartly and conservatively, bring photo ID.
-A small pause at the beginning to collect your thoughts and then begin (definitely not the first words/expletives that come into your head).
-No wild gesticulations - hands clasped under the table - use the pen/pencil to make the relevant diagram then hands back under the table, not fiddling with the pencil.
-Don't dig a hole - if you don't know, say so.
-Don't mention something you can't talk about i.e. eponymous syndromes.
-Don't say: "You would intubate....etc" It apparantly annoys examiners - they will not be doing anything apart from marking. Say: "I would intubate..." or "The patient requires intubation"
-Don't use abbreviations or colloquialisms. You need to sound professional.
-Be able to draw all line diagrams from the A to Z.
-Learn to succinctly summarise the long case history - do not simply repeat the information given on the sheet.
Lastly, try and smile. You may want to scream/cry/run away/attack the examiner/soil yourself but a calm exterior belies the autonomic and emotional surges simmering under the surface, it implies you're human, and just may save you.
Good luck!!
It has been such a rollercoaster ride during viva practices. There are some sessions where I am concise, calm, and knowledgeable, then there are the ones where I have completely crumpled and been close to tears with frustration at having such a poor memory. Actually, there are a few words of advice I would like to impart, both from experience of preparation and the day itsself.
The next week
-Don't overdo it - you can't read whole textbooks in one day. Plan sensibly.
-Another piece of excellent advice I was given, is to imagine that the structure of your answer is analogous to a tree. Do not aim for the fruit immediately - start with the trunk (or DEFINITION) and a few main branches thereafter (CLASSIFY). The examiner will guide you towards which piece of fruit to pick and digest upon!!
-Learn to classify drugs. I use Sasada & Smith which breaks them up nicely into different categories.
-Always talk about drugs in terms of dose by weight e.g. 5mg/kg rather that 150mg (especially in paediatrics.
-Try not to A-Z chase - you know the sport. Open the A to Z and read a topic, then see a boldly outlined word so turn to that topic etc etc. You'll be there for ever.
-Make sure you can interpret and describe ECGs/CXR/basic CT etc.
-Refamiliarise yourself with some recent guidelines/topics. most have been mentioned previously in this blog.
-Have a look at the RCOA Finals Guide - just occaisionally some of the Short Cases/Long Cases/Basic Science stuff comes up word for word.
On the day
-Usual advice of arrive early, dress smartly and conservatively, bring photo ID.
-A small pause at the beginning to collect your thoughts and then begin (definitely not the first words/expletives that come into your head).
-No wild gesticulations - hands clasped under the table - use the pen/pencil to make the relevant diagram then hands back under the table, not fiddling with the pencil.
-Don't dig a hole - if you don't know, say so.
-Don't mention something you can't talk about i.e. eponymous syndromes.
-Don't say: "You would intubate....etc" It apparantly annoys examiners - they will not be doing anything apart from marking. Say: "I would intubate..." or "The patient requires intubation"
-Don't use abbreviations or colloquialisms. You need to sound professional.
-Be able to draw all line diagrams from the A to Z.
-Learn to succinctly summarise the long case history - do not simply repeat the information given on the sheet.
Lastly, try and smile. You may want to scream/cry/run away/attack the examiner/soil yourself but a calm exterior belies the autonomic and emotional surges simmering under the surface, it implies you're human, and just may save you.
Good luck!!
Monday, 17 November 2008
Heading for London
Sorry about lack of posting in last week or so - have been 3rd on-call in theatre with some pretty hectic shifts - all good experience (met someone with CREST syndrome yesterday - anyone remember that from medical finals?? As with all syndromes, potentially difficult airway which thankfully for us turned out to be relatively straightforward). Anyway, I'm digressing so back to the point.
I passed the written paper (much relief!) - congratulations to everyone else who did. So, we have three weeks of intense viva practice ahead. Make sure you pester all of your colleagues at work to viva you - try and focus in on their specialist interests as they will have more to offer. There are usually a few secret physics and statistics whizzkids hiding in each department too!
Today, I thought I would mention investigations. I got slightly caught out during my last clinical viva when asked about FBC and the various indices, and about sickledex testing, so it's worth having a quick look at a few basic investigations.
FBC
-RBC Count: the number of red cells in the blood.
-Hb: concentration of HB protein in blood. Normal values: 12 to 18 g/dL of blood but are influenced by the age, sex and ethnic origin in the person.
-PCV (Hct): % of total blood volume occupied by red cells. The haematocrit is the proportion, by volume, of the blood that consists of red blood cells post-centrifugation.
-MCV: mean volume of red cells. Normal range 82-98 fl
-MCH: mean amount of Hb in red cells. Normal range 26-34 pg
-MCHC: mean concentration of Hb in red cells. Normal range 31-37 g/dl
-RDW: red cell distribution width (measure of variation of RBC population). Normal range 11.5-14.5%
Haemostasis/Clotting
-APTT: activated partial thromboplastin time measures efficacy of contact activation (formerly intrinsic) and common coagulation pathways. Monitors effective heparin treatment.
-PT: prothrombin time determines clotting tendencies of blood (formerly extrinsic pathway measurement). Trends useful in measuring efficacy of warfarin treatment & progress of liver damage. INR derived from PT: ratio of pt's PT to control sample (raised to power of specific sensitivity index).
-Platelet function: bleeding time & thromboelastography (a measure of clot formation speed and clot strength)
Sicle Cell Testing
-Sickledex (or sickle solubility testing): a blood sample is added to a reducing solution (e.g. sodium dithionite). HbS will give a turbid appearance whilst HbA will give a clear solution. Remember that this test does not distinguish between HbSA and HbSS, merely the presence of the sickle gene.
-Hb electrophoresis: different types of Hb move at different speeds along the gel. Can confirm with high-performance liquid chromatography.
Biochemistry
-HbA1c: Glycosylated Hb identifies average blood glucose conc over period of time. Measured by chromatography or immunoassay. The International Diabetes Federation and American College of Endocrinology recommend HbA1c values below 6.5% (Normal ref range: 4-5.9%).
-Urea: product of amino acid breakdown to ammonia which is produced in the urea cycle. It is filtered freely at the glomerulus and approx. half is reabsorbed in the PCT. Responsible for the majority of daily nitrogen excretion.
-Creatinine: Formed constantly from phosphorylcreatine in skeletal muscle. It is freely filtered by the glomerulus, but also actively secreted by the renal tubules in very small amounts such that creatinine clearance overestimates actual GFR by 10-20%. However, the values agree quite well with the GFR values measured with inulin because the value for plasma creatinine concentration is also high as a result of nonspecific substances, cancelling out the error.
-Troponins: Trop I, C, T are three protein sub-units of larger troponin complex. Trop C binds to Ca2+ leading to conformational change in Trop I. Trop T binds other troponin components to tropomyosin forming a complex. Trop I binds to actin to hold the previous complex in place by inhibiting ATP activity. Trop I & T are not normally found in plasma, but raised levels are v.sensitive/specific indicators of cardiac damage and differentiate between unstable angina & MI. Troponin C is not used to measure myocardial damage as this isoform is shared with skeletal muscle, rendering it non-specific. Levels are measured by immunoassay methods.
I passed the written paper (much relief!) - congratulations to everyone else who did. So, we have three weeks of intense viva practice ahead. Make sure you pester all of your colleagues at work to viva you - try and focus in on their specialist interests as they will have more to offer. There are usually a few secret physics and statistics whizzkids hiding in each department too!
Today, I thought I would mention investigations. I got slightly caught out during my last clinical viva when asked about FBC and the various indices, and about sickledex testing, so it's worth having a quick look at a few basic investigations.
FBC
-RBC Count: the number of red cells in the blood.
-Hb: concentration of HB protein in blood. Normal values: 12 to 18 g/dL of blood but are influenced by the age, sex and ethnic origin in the person.
-PCV (Hct): % of total blood volume occupied by red cells. The haematocrit is the proportion, by volume, of the blood that consists of red blood cells post-centrifugation.
-MCV: mean volume of red cells. Normal range 82-98 fl
-MCH: mean amount of Hb in red cells. Normal range 26-34 pg
-MCHC: mean concentration of Hb in red cells. Normal range 31-37 g/dl
-RDW: red cell distribution width (measure of variation of RBC population). Normal range 11.5-14.5%
Haemostasis/Clotting
-APTT: activated partial thromboplastin time measures efficacy of contact activation (formerly intrinsic) and common coagulation pathways. Monitors effective heparin treatment.
-PT: prothrombin time determines clotting tendencies of blood (formerly extrinsic pathway measurement). Trends useful in measuring efficacy of warfarin treatment & progress of liver damage. INR derived from PT: ratio of pt's PT to control sample (raised to power of specific sensitivity index).
-Platelet function: bleeding time & thromboelastography (a measure of clot formation speed and clot strength)
Sicle Cell Testing
-Sickledex (or sickle solubility testing): a blood sample is added to a reducing solution (e.g. sodium dithionite). HbS will give a turbid appearance whilst HbA will give a clear solution. Remember that this test does not distinguish between HbSA and HbSS, merely the presence of the sickle gene.
-Hb electrophoresis: different types of Hb move at different speeds along the gel. Can confirm with high-performance liquid chromatography.
Biochemistry
-HbA1c: Glycosylated Hb identifies average blood glucose conc over period of time. Measured by chromatography or immunoassay. The International Diabetes Federation and American College of Endocrinology recommend HbA1c values below 6.5% (Normal ref range: 4-5.9%).
-Urea: product of amino acid breakdown to ammonia which is produced in the urea cycle. It is filtered freely at the glomerulus and approx. half is reabsorbed in the PCT. Responsible for the majority of daily nitrogen excretion.
-Creatinine: Formed constantly from phosphorylcreatine in skeletal muscle. It is freely filtered by the glomerulus, but also actively secreted by the renal tubules in very small amounts such that creatinine clearance overestimates actual GFR by 10-20%. However, the values agree quite well with the GFR values measured with inulin because the value for plasma creatinine concentration is also high as a result of nonspecific substances, cancelling out the error.
-Troponins: Trop I, C, T are three protein sub-units of larger troponin complex. Trop C binds to Ca2+ leading to conformational change in Trop I. Trop T binds other troponin components to tropomyosin forming a complex. Trop I binds to actin to hold the previous complex in place by inhibiting ATP activity. Trop I & T are not normally found in plasma, but raised levels are v.sensitive/specific indicators of cardiac damage and differentiate between unstable angina & MI. Troponin C is not used to measure myocardial damage as this isoform is shared with skeletal muscle, rendering it non-specific. Levels are measured by immunoassay methods.
Saturday, 8 November 2008
It's Good To Talk
The weather is getting colder, the nights longer, and we're still waiting for the results of the written exam. It can only mean one thing: it's viva season!
Hopefully most of us have started getting viva practice - if not, don't wait until next Friday. Find some consultants/senior registrars or anyone who has taken the exam and get talking to them. Ask them what cases they got given and get them to viva you on those topics. Some people find getting a viva group together if there are a couple of you in the same hospital/deanery, and grilling each other.
On the day, there are two sets of vivas:
-Clinical viva: 50 minutes, comprising 20 minutes of long case questioning (there is a period of time beforehand to peruse the case and construct potential answers - writing down stuff is allowed) followed by three short cases.
-Clinical science viva: 30 minutes on physiology, physics & clinical measurement, anatomy, and pharmacology in equal aliquots.
There is plenty of practice viva material to be found for your enjoyment!:
AnaesthesiaUK have a large database of past questions sent in by candidates here & here.
I have grouped all of their questions according to viva type:
-Basic Sciences
-Long Cases
-Short Cases
Again, topical items have come up in the past in some guise or another. For instance, placenta, pleura, COX-2 inhibitors & heart disease, CPEX testing to name but a few. So keep reading the bulletins, CEACCP articles and review articles from the journals.
Remember, do not ignore Basic Sciences!
Hopefully most of us have started getting viva practice - if not, don't wait until next Friday. Find some consultants/senior registrars or anyone who has taken the exam and get talking to them. Ask them what cases they got given and get them to viva you on those topics. Some people find getting a viva group together if there are a couple of you in the same hospital/deanery, and grilling each other.
On the day, there are two sets of vivas:
-Clinical viva: 50 minutes, comprising 20 minutes of long case questioning (there is a period of time beforehand to peruse the case and construct potential answers - writing down stuff is allowed) followed by three short cases.
-Clinical science viva: 30 minutes on physiology, physics & clinical measurement, anatomy, and pharmacology in equal aliquots.
There is plenty of practice viva material to be found for your enjoyment!:
AnaesthesiaUK have a large database of past questions sent in by candidates here & here.
I have grouped all of their questions according to viva type:
-Basic Sciences
-Long Cases
-Short Cases
Again, topical items have come up in the past in some guise or another. For instance, placenta, pleura, COX-2 inhibitors & heart disease, CPEX testing to name but a few. So keep reading the bulletins, CEACCP articles and review articles from the journals.
Remember, do not ignore Basic Sciences!
Sunday, 26 October 2008
A Long Week
A lot of interesting thoughts after the written exam on Tuesday. The SAQ paper is available to look at online now here.
SAQ paper
Yet again there was a proportion of this paper which could have and was predicted by various sources. I don't think it was an overly tricky exam - the hardest part of it is the time pressure you have to write each question.
1) Morbid obesity - straight from the Association of Anaesthetists Guidelines published in 2007. Enforces the need to read these guidelines in revision, as highlighted in the previous posting on sexy topics. Note the inclusion of the organisational section - requiring us to think from a managerial viewpoint, not just clinical. There has been a recent article in CEACCP October 2008 (incidentally after the paper was written) on morbid obesity.
2) Sciatic Nerve Block - standard anatomy question. I mentioned the sciatic nerve blocks (amongst others) in my anatomy posting at the beginning of September as a topic to learn.
3) GA LSCS in woman with ASD - difficult to predict this type of question. Requires knowledge of cardiac shunts and perioperative physiology/pharmacology for GA LSCS.
4) Subclavian Vein Cannulation - a surprising repeat question from October 2007 due to it being done very well last time. In fact, I suspect the reason why it came up was due to the infection component of the question - a recurring theme in this exam and something which I have touched upon in previous postings.
5) Study Design - I have no comment to make on this question.
6) PONV/Dystonic reaction - PONV is a standard question covered in Bricker and other texts. I had to delve into some past A&E experience for the dystonic reaction which was slightly random but I guess those who have seen it post-drug administration would not forget it.
7) Burns - Standard question. I must remember that 40 x 70 is not 2100 - duh!
8) Fat Embolism - at first site quite a random question, however it was a CEACCP article in October 2007 highlighting the value of reading these publications as part of the exam revision. Thanks to Dr M, one of my previous colleagues, who provided the best laugh in the pub afterwards with his explanation of minimising fat embolism by using a seatbelt!!
9) Brain Stem Death - quite crafty, not requiring the usual 'what do you test' etc. I found it quite tricky to answer, despite having looked after exactly such a patient the week before. It will be a matter of hoping that your key words match those on the marking sheet!
10) Child Abuse - more of a general exam question which could turn up in a Paeds/A&E/GP exam in almost identical format. It's inclusion was probably as a 'trendy topic' highlighting our need as anaesthetists to be aware of such issues. Luck hasn't been with me in the past taking this exam, but my participation in a Child Abuse mandatory training seminar two weeks ago has certainly scored me some points here!
11) Infection Transmission - If you had read the publication of updated guidelines on Infection Control in Anaesthesia (September 2008 edition of Anaesthesia p.1027) by the Association of Anaesthetists, you should have been laughing for this one. I posted about this topic at the end of August.
12) Rheumatoid Arthritis another standard question found in most anaesthesia exam texts. There was a CEACCP article in December 2006.
MCQ
Again, difficult to assess any sort of achievement in this section of the exam. Of note, there were 13-14 questions straight from the College guide, highlighting the importance of doing these practice papers.
Hope you've all had a good few days off - time to start thinking about some viva practice!
SAQ paper
Yet again there was a proportion of this paper which could have and was predicted by various sources. I don't think it was an overly tricky exam - the hardest part of it is the time pressure you have to write each question.
1) Morbid obesity - straight from the Association of Anaesthetists Guidelines published in 2007. Enforces the need to read these guidelines in revision, as highlighted in the previous posting on sexy topics. Note the inclusion of the organisational section - requiring us to think from a managerial viewpoint, not just clinical. There has been a recent article in CEACCP October 2008 (incidentally after the paper was written) on morbid obesity.
2) Sciatic Nerve Block - standard anatomy question. I mentioned the sciatic nerve blocks (amongst others) in my anatomy posting at the beginning of September as a topic to learn.
3) GA LSCS in woman with ASD - difficult to predict this type of question. Requires knowledge of cardiac shunts and perioperative physiology/pharmacology for GA LSCS.
4) Subclavian Vein Cannulation - a surprising repeat question from October 2007 due to it being done very well last time. In fact, I suspect the reason why it came up was due to the infection component of the question - a recurring theme in this exam and something which I have touched upon in previous postings.
5) Study Design - I have no comment to make on this question.
6) PONV/Dystonic reaction - PONV is a standard question covered in Bricker and other texts. I had to delve into some past A&E experience for the dystonic reaction which was slightly random but I guess those who have seen it post-drug administration would not forget it.
7) Burns - Standard question. I must remember that 40 x 70 is not 2100 - duh!
8) Fat Embolism - at first site quite a random question, however it was a CEACCP article in October 2007 highlighting the value of reading these publications as part of the exam revision. Thanks to Dr M, one of my previous colleagues, who provided the best laugh in the pub afterwards with his explanation of minimising fat embolism by using a seatbelt!!
9) Brain Stem Death - quite crafty, not requiring the usual 'what do you test' etc. I found it quite tricky to answer, despite having looked after exactly such a patient the week before. It will be a matter of hoping that your key words match those on the marking sheet!
10) Child Abuse - more of a general exam question which could turn up in a Paeds/A&E/GP exam in almost identical format. It's inclusion was probably as a 'trendy topic' highlighting our need as anaesthetists to be aware of such issues. Luck hasn't been with me in the past taking this exam, but my participation in a Child Abuse mandatory training seminar two weeks ago has certainly scored me some points here!
11) Infection Transmission - If you had read the publication of updated guidelines on Infection Control in Anaesthesia (September 2008 edition of Anaesthesia p.1027) by the Association of Anaesthetists, you should have been laughing for this one. I posted about this topic at the end of August.
12) Rheumatoid Arthritis another standard question found in most anaesthesia exam texts. There was a CEACCP article in December 2006.
MCQ
Again, difficult to assess any sort of achievement in this section of the exam. Of note, there were 13-14 questions straight from the College guide, highlighting the importance of doing these practice papers.
Hope you've all had a good few days off - time to start thinking about some viva practice!
Monday, 20 October 2008
Good Luck!!
**Apologies for the mistake earlier - the written exam in London is at the Royal National Hotel, not the RCOA as I wrote earlier.***
My advice, for what it's worth at this late stage, is:
-Try not to panic - part of this exam is keeping a cool head. Remember that the minimum needed to pass the SAQ is usually 12/20 on each question (sometimes lower, sometimes higher) to get a '2', and minimum 6 1+'s and 6 2's (or even 3 2+'s and 9 1+'s although not advised).
-Get nice pens, plus a spare or two
-Plan your journey and leave time to spare.
-Arrive early & bring photo ID as told.
-Read the questions (properly).
-Write nicely and space answers out - make it easy for the examiner! 10% of marks can be gained here!
-Don't overrun on questions.
-Eat and sleep well tonight!
-Look through RCOA MCQs
-Look through some guidelines/protocols/past papers.
-Have some luck !
All the best and I'll see you Londoners tomorrow for a beer at about 16:50!!
James
My advice, for what it's worth at this late stage, is:
-Try not to panic - part of this exam is keeping a cool head. Remember that the minimum needed to pass the SAQ is usually 12/20 on each question (sometimes lower, sometimes higher) to get a '2', and minimum 6 1+'s and 6 2's (or even 3 2+'s and 9 1+'s although not advised).
-Get nice pens, plus a spare or two
-Plan your journey and leave time to spare.
-Arrive early & bring photo ID as told.
-Read the questions (properly).
-Write nicely and space answers out - make it easy for the examiner! 10% of marks can be gained here!
-Don't overrun on questions.
-Eat and sleep well tonight!
-Look through RCOA MCQs
-Look through some guidelines/protocols/past papers.
-Have some luck !
All the best and I'll see you Londoners tomorrow for a beer at about 16:50!!
James
Saturday, 18 October 2008
Let The Fun & Games Commence
How are you all feeling? The following sound familiar?
-Frantically trying to read through whole text books in half a day
-A to Z word chasing (you know the one - you read something in the A to Z, you see another word that is highlighted, you go to that entry, and so on....and on).
-Getting worse marks in the MCQs than when you started revising.
-Slight sick feeling that you should have started revising earlier.
-Other half completely fed up with you
I'm sure you get the picture! The weekend before the exam starts is horrible. It feels like there is a lot to get through, but the awful truth is (with the exception of a few jammy people) most of what is read this weekend will make no difference at all on Tuesday. In fact, the last time I sat this exam, I could have done the majority of the SAQ paper months previously and it wouldn't have changed my marks grossly. Sick isn't it?
So, what to do for two and a bit days? Everyone will be different but here's what I'm attempting to do in no particular order:
-Anatomy (there will almost certainly be one SAQ - learn the diagrams!) - done today.
-Bricker SAQ book
-The new Guide to the FRCA Final examination MCQs & SAQs (it's a new edition - some MCQs will come up and there may even be SAQs as well)
-Some sexy topics (see earlier postings)
-A quick flick through some old RCOA SAQs
-If not already done, consider having a go at the practice paper I set out in an earlier posting.
-Frantically trying to read through whole text books in half a day
-A to Z word chasing (you know the one - you read something in the A to Z, you see another word that is highlighted, you go to that entry, and so on....and on).
-Getting worse marks in the MCQs than when you started revising.
-Slight sick feeling that you should have started revising earlier.
-Other half completely fed up with you
I'm sure you get the picture! The weekend before the exam starts is horrible. It feels like there is a lot to get through, but the awful truth is (with the exception of a few jammy people) most of what is read this weekend will make no difference at all on Tuesday. In fact, the last time I sat this exam, I could have done the majority of the SAQ paper months previously and it wouldn't have changed my marks grossly. Sick isn't it?
So, what to do for two and a bit days? Everyone will be different but here's what I'm attempting to do in no particular order:
-Anatomy (there will almost certainly be one SAQ - learn the diagrams!) - done today.
-Bricker SAQ book
-The new Guide to the FRCA Final examination MCQs & SAQs (it's a new edition - some MCQs will come up and there may even be SAQs as well)
-Some sexy topics (see earlier postings)
-A quick flick through some old RCOA SAQs
-If not already done, consider having a go at the practice paper I set out in an earlier posting.
Tuesday, 14 October 2008
Disaster
We are having a new boiler installed at the moment, which is just as well because it's freezing! I was helping to move a bookcase for the plumbers who wanted access to an under-floor area when the bookcase collapsed........on my thumb........on my right hand!
Firstly, the negatives: the £$*&@@^ A-delta & C-fibres were the last thing on my mind at that point as I performed what was probably a comedy ACME cartoon dance holding my throbbing thumb. Then, I realised the potential problem of the little test which involves a small amount of scribbling next week - could I learn to write left-handed in one week? Unlikely. Would I have to pray that I have the healing powers of the hot cheerleader on Heroes? Most likely. It kind of scuppers my plans of doing lots of practice SAQs this week though.
Lastly, the positives: I don't have to do any practice SAQs this week...... Hmmm - great attitude! Seriously though, I did manage to do the practice exam which I posted last week. I sat down and did the whole lot in almost three hours exactly so my timing shouldn't be too much of a problem. I give myself about 35 minutes to plans for all 12 questions. I take 3 pieces of blank A4 paper, divide them in half horizontally and write my 12 plans in each section. I then look at all the questions and decide on an order to do them in, starting first with the questions I find easiest/know the most about, and ending with the weaker questions. I find that this gives me some confidence at the beginning and I find my writing flow. I'll spend 10-11 minutes per question rigidly and then move on. The hardest section of the exam for me is concentrating on and writing the last four questions - your hand hurts and your mind is tired and wandering. That's why you need to train yourself by doing lots of full papers. Judging by a couple of postings on Doctors.net we're all extremely fed up now. We're nearly there - it's often a battle of the mind at this point because we've done most of the leg-work - so keep going and I'll look forward to sharing a beer with you all next Tuesday evening!!
Below is a picture which describes my thumb, and also should describe how we're all feeling too!!

Firstly, the negatives: the £$*&@@^ A-delta & C-fibres were the last thing on my mind at that point as I performed what was probably a comedy ACME cartoon dance holding my throbbing thumb. Then, I realised the potential problem of the little test which involves a small amount of scribbling next week - could I learn to write left-handed in one week? Unlikely. Would I have to pray that I have the healing powers of the hot cheerleader on Heroes? Most likely. It kind of scuppers my plans of doing lots of practice SAQs this week though.
Lastly, the positives: I don't have to do any practice SAQs this week...... Hmmm - great attitude! Seriously though, I did manage to do the practice exam which I posted last week. I sat down and did the whole lot in almost three hours exactly so my timing shouldn't be too much of a problem. I give myself about 35 minutes to plans for all 12 questions. I take 3 pieces of blank A4 paper, divide them in half horizontally and write my 12 plans in each section. I then look at all the questions and decide on an order to do them in, starting first with the questions I find easiest/know the most about, and ending with the weaker questions. I find that this gives me some confidence at the beginning and I find my writing flow. I'll spend 10-11 minutes per question rigidly and then move on. The hardest section of the exam for me is concentrating on and writing the last four questions - your hand hurts and your mind is tired and wandering. That's why you need to train yourself by doing lots of full papers. Judging by a couple of postings on Doctors.net we're all extremely fed up now. We're nearly there - it's often a battle of the mind at this point because we've done most of the leg-work - so keep going and I'll look forward to sharing a beer with you all next Tuesday evening!!
Below is a picture which describes my thumb, and also should describe how we're all feeling too!!

Sunday, 5 October 2008
COX-2 Inhibitors
I believe that a couple candidates were asked in the last set of vivas about controversy surrounding COX-2 inhibitors. Here are some things to think about:
-The first controversy was with Rofecoxib (Vioxx) marketed by Merck & Co.
-Approved by the FDA in 1999 as an analgesic for treatment of osteoarthritis and various other acute pain conditions - by being a selective COX inhibitor, gastric side-effects e.g. ulceration were thought to be avoided.
-Over the next few years, concern grew about potential serious cardiovascular side-effects in patients who were taking rofecoxib.
-In 2001, the VIGOR study(Vioxx GI Outcomes Research) (Bombardier et al) was submitted to the FDA. It compared rofecoxib and naproxen, looking at efficacy and side effects over a one year period.
-They found a statistically significant 4-fold increased risk of acute MI in rofecoxib patients who were already at increased risk of cardiovascular disease, when compared to naproxen patients.
-The proposed mechanisms of cardiotoxicity included inhibition of PGI2 (prostacyclin), which is normally involved in vasodilatation & clot formation prevention, and possibly the production of cardiotoxic metabolites from rofecoxib itsself.
-There was further controversy between Merck & Co and the NEJM regarding certain data being withheld which resulted in lengthy legal proceedings.
-In 2002, warning labels were produced on rofecoxib packaging warning of the increased risk of CVS morbidity.
-Since then, further studies have demonstrated higher rates of CVS morbidity in Vioxx patients e.g. MI, CVA, arrhythmia, renovascular disease
-Rofecoxib was withdrawn in 2004 by Merck & Co.
The second controversy was with Valdecoxib (Bextra), manufactured by G.D.Searle & Company (now part of Pfizer) and approved by the FDA in 2001.
-Again, it was used to treat OA, RA, and painful menstruation.
-It was withdrawn in 2005 due to a perceived increased risk of MI & CVA. Also, Toxic Epidermal Necrolysis and Steven Johnson's Syndrome had been reported.
-So what has been learned from this:
Doctors must be selective when prescribing COX-2 inhibitors both in dose and duration, especially to those with an increased risk/previous history of cardiovascular disease.
New drugs with mechanisms of action similar to COX-2 inhibitors, including the COX-2 inhibitors themsselves will undergo much more extensive trials in the future, to try and avoid both the medical and financial problems associated with rofecoxib.
-The first controversy was with Rofecoxib (Vioxx) marketed by Merck & Co.
-Approved by the FDA in 1999 as an analgesic for treatment of osteoarthritis and various other acute pain conditions - by being a selective COX inhibitor, gastric side-effects e.g. ulceration were thought to be avoided.
-Over the next few years, concern grew about potential serious cardiovascular side-effects in patients who were taking rofecoxib.
-In 2001, the VIGOR study(Vioxx GI Outcomes Research) (Bombardier et al) was submitted to the FDA. It compared rofecoxib and naproxen, looking at efficacy and side effects over a one year period.
-They found a statistically significant 4-fold increased risk of acute MI in rofecoxib patients who were already at increased risk of cardiovascular disease, when compared to naproxen patients.
-The proposed mechanisms of cardiotoxicity included inhibition of PGI2 (prostacyclin), which is normally involved in vasodilatation & clot formation prevention, and possibly the production of cardiotoxic metabolites from rofecoxib itsself.
-There was further controversy between Merck & Co and the NEJM regarding certain data being withheld which resulted in lengthy legal proceedings.
-In 2002, warning labels were produced on rofecoxib packaging warning of the increased risk of CVS morbidity.
-Since then, further studies have demonstrated higher rates of CVS morbidity in Vioxx patients e.g. MI, CVA, arrhythmia, renovascular disease
-Rofecoxib was withdrawn in 2004 by Merck & Co.
The second controversy was with Valdecoxib (Bextra), manufactured by G.D.Searle & Company (now part of Pfizer) and approved by the FDA in 2001.
-Again, it was used to treat OA, RA, and painful menstruation.
-It was withdrawn in 2005 due to a perceived increased risk of MI & CVA. Also, Toxic Epidermal Necrolysis and Steven Johnson's Syndrome had been reported.
-So what has been learned from this:
Doctors must be selective when prescribing COX-2 inhibitors both in dose and duration, especially to those with an increased risk/previous history of cardiovascular disease.
New drugs with mechanisms of action similar to COX-2 inhibitors, including the COX-2 inhibitors themsselves will undergo much more extensive trials in the future, to try and avoid both the medical and financial problems associated with rofecoxib.
Friday, 3 October 2008
Time yourself
I've not posted for a while due to a hectic ICU schedule and also because I've been trying to do some serious work.
Many thanks to Dr Booker who runs the infamous Booker Course up in Liverpool, who mentioned this website as a useful source of information for Finals revision. I went on this course last March and, apart from scaring the hell out of me, it really dragged me up to the level required to pass the SAQ section of the written paper. More than anything, it gave me a method and structure which provided me with confidence to tackle and complete the paper within the allotted time-frame.
I thought I would follow up my last posting about sexy topics with an equally sexy mock-exam to try. You will recognise some of the questions, some are topical, and some I have written myself - apologies if they are poorly worded. Of vital importance is that you have a clear 3 hour period to attempt the exam, and stick to the timings for each question. Hopefully by now you should have some idea of your preferred method for answering the SAQs and should have practiced some timed questions. Try this one seriously as if it were the paper.
Question 1
a) Describe the factors that may lead to i) venous air embolism (20%) and ii) arterial air embolism (20%)
b) What is paradoxical air embolism and how does it occur? (20%)
c) Explain the physiological basis for the use of capnography in the detection of venous air embolism. (30%)
Question 2
A 4 year old (20 kg) is admitted with acute appendicitis and is scheduled for urgent surgery. She has been vomiting for 2 days, is pyrexial, has a tachycardia of 170 bpm and prolonged capillary refill.
a) Describe the perioperative fluid management of this case using intravenous crystalloids. (60%)
b) Outline the complications that can occur with inappropriate intravenous crystalloid therapy. (30%)
Question 3
a) What are the important considerations in the preoperative assessment of a hypertensive patient presenting for elective surgery? (50%)
b) Outline the perioperative risks associated with hypertension and their management. (40%)
Question 4
a) Briefly describe your technique for performing a deep cervical plexus block for carotid
endarterectomy under local anaesthesia. (35%)
b) List the complications of a deep cervical plexus block. (35%)
c) List the advantages and disadvantages of performing a carotid endarterectomy under regional
anaesthesia. (30%)
Question 5
a) How is ventilator-associated pneumonia (VAP) diagnosed? (20%)
b) Explain the i) physical (50%) ii) positional (15%) and iii) pharmacological (15%) strategies that have been advocated for its prevention?
Question 6
a) List the specific problems and risks associated with a twin pregnancy. (45%)
b) What are the important considerations and options when planning the anaesthetic management for the delivery of twins around term? (45%)
Question 7
a) If neuromuscular block has been achieved during general anaesthesia using rocuronium explain the mechanism of spontaneous recovery from neuromuscular blockade. (15%)
b) What classes of drugs could be used to accelerate the recovery from rocuronium? (10%)
c) How do the classes of drugs in part (b) work? (15%)
d) What are the advantages and disadvantages of the classes of drugs identified in part (b)? (50%)
Question 8
a) List the complications arising from anaesthesia in the prone position (60%)
b) How may these be avoided? (40%)
Question 9
You are performing an axillary nerve block for a 54 year old man pre-hand surgury. After injecting 15mls 0.375% bupivacaine, the man develops an acute tonic-clonic seizure quickly followed by loss of consciousness and ventricular fibrillation on the ECG monitor.
a) Describe your immediate management and resuscitation (30%)
b) Assuming this man has developed LA toxicity, outline your further treatment (70%)
Question 10
a) What are the current clinical indications for perioperative blood transfusion? (40%)
b) Outline methods of reducing perioperative autologous blood transfusion (60%)
Question 11
a) Describe the pharmacology of gabapentin (60%)
b) List it's current clinical uses. (40%)
Question 12
(a) Define explicit and implicit awareness during general anaesthesia. (10%)
(b) What may increase the likelihood of awareness? (40%)
(c) List the techniques used to assess depth of anaesthesia and comment on their value. (40%)
Now get a couple of consultants/registrars to mark your questions - Good Luck!!
Many thanks to Dr Booker who runs the infamous Booker Course up in Liverpool, who mentioned this website as a useful source of information for Finals revision. I went on this course last March and, apart from scaring the hell out of me, it really dragged me up to the level required to pass the SAQ section of the written paper. More than anything, it gave me a method and structure which provided me with confidence to tackle and complete the paper within the allotted time-frame.
I thought I would follow up my last posting about sexy topics with an equally sexy mock-exam to try. You will recognise some of the questions, some are topical, and some I have written myself - apologies if they are poorly worded. Of vital importance is that you have a clear 3 hour period to attempt the exam, and stick to the timings for each question. Hopefully by now you should have some idea of your preferred method for answering the SAQs and should have practiced some timed questions. Try this one seriously as if it were the paper.
Question 1
a) Describe the factors that may lead to i) venous air embolism (20%) and ii) arterial air embolism (20%)
b) What is paradoxical air embolism and how does it occur? (20%)
c) Explain the physiological basis for the use of capnography in the detection of venous air embolism. (30%)
Question 2
A 4 year old (20 kg) is admitted with acute appendicitis and is scheduled for urgent surgery. She has been vomiting for 2 days, is pyrexial, has a tachycardia of 170 bpm and prolonged capillary refill.
a) Describe the perioperative fluid management of this case using intravenous crystalloids. (60%)
b) Outline the complications that can occur with inappropriate intravenous crystalloid therapy. (30%)
Question 3
a) What are the important considerations in the preoperative assessment of a hypertensive patient presenting for elective surgery? (50%)
b) Outline the perioperative risks associated with hypertension and their management. (40%)
Question 4
a) Briefly describe your technique for performing a deep cervical plexus block for carotid
endarterectomy under local anaesthesia. (35%)
b) List the complications of a deep cervical plexus block. (35%)
c) List the advantages and disadvantages of performing a carotid endarterectomy under regional
anaesthesia. (30%)
Question 5
a) How is ventilator-associated pneumonia (VAP) diagnosed? (20%)
b) Explain the i) physical (50%) ii) positional (15%) and iii) pharmacological (15%) strategies that have been advocated for its prevention?
Question 6
a) List the specific problems and risks associated with a twin pregnancy. (45%)
b) What are the important considerations and options when planning the anaesthetic management for the delivery of twins around term? (45%)
Question 7
a) If neuromuscular block has been achieved during general anaesthesia using rocuronium explain the mechanism of spontaneous recovery from neuromuscular blockade. (15%)
b) What classes of drugs could be used to accelerate the recovery from rocuronium? (10%)
c) How do the classes of drugs in part (b) work? (15%)
d) What are the advantages and disadvantages of the classes of drugs identified in part (b)? (50%)
Question 8
a) List the complications arising from anaesthesia in the prone position (60%)
b) How may these be avoided? (40%)
Question 9
You are performing an axillary nerve block for a 54 year old man pre-hand surgury. After injecting 15mls 0.375% bupivacaine, the man develops an acute tonic-clonic seizure quickly followed by loss of consciousness and ventricular fibrillation on the ECG monitor.
a) Describe your immediate management and resuscitation (30%)
b) Assuming this man has developed LA toxicity, outline your further treatment (70%)
Question 10
a) What are the current clinical indications for perioperative blood transfusion? (40%)
b) Outline methods of reducing perioperative autologous blood transfusion (60%)
Question 11
a) Describe the pharmacology of gabapentin (60%)
b) List it's current clinical uses. (40%)
Question 12
(a) Define explicit and implicit awareness during general anaesthesia. (10%)
(b) What may increase the likelihood of awareness? (40%)
(c) List the techniques used to assess depth of anaesthesia and comment on their value. (40%)
Now get a couple of consultants/registrars to mark your questions - Good Luck!!
Wednesday, 17 September 2008
Sexy Topics
Certain topics have a propensity to appear in the Final Examination. Some are topical, some are even newsworthy, and some have been done badly in previous exam sittings. Is it worth trying to spot some questions? Absolutely; we successfully managed to 'guess' 3-4 questions in the last exam, so I'm going to list a few topics which I think may come up for various reasons.
Previous SAQs done badly as highlighted in the Examiner's Report
- Preop assessment of a hypertensive patient (October 2007 SAQ paper)
- Management of twins (October 2007 SAQ paper)
- Air Embolus (April 2008 SAQ paper)
- Paediatric Fluid Balance (April 2008 SAQ paper)
- Neuromuscular Blocking Reversal + Sugammadex (April 2008 SAQ paper)
Other topics include issues of public interest and patient safety which were highlighted in the Examiner's report as being repeatedly done badly and therefore will continue to be represented in the examination, guidelines (including AAGBI, NICE, NPSA), and review articles from major journals.
-Awareness: continually remains in the public eye
-Healthcare-associated infections (VIP cannula scores/MRSA/C.Diff): huge at present also linked with recent publication by the aagbi on Infection in Anaesthesia
-CEMACH - easily repeated question
-Mental Capacity Act - has come into force in late 2007. This is the link I used previously, but for much more comprehensive coverage of both this and issues of Consent, EI has done a fantastic job putting togther some very simple explanations of tricky topics!
-LA toxicity +/- Intralipid use - it's going to come up eventually
-Malignant Hyperthermia treatment
-Blood Transfusion
-Perioperative Management of the Morbidly Obese Patient
-Prophylaxis against Infective Endocarditis: NICE March 2008
-Perioperative hypothermia: NICE April 2008
-Head Injury: NICE September 2007
-VAP: NICE August 2008
-CEPEX testing here
-POISE (Perioperative Ischaemic Evaluation) study: looks at beta-blocker use in non-cardiac surgery
-Amniotic Fluid Embolism: inexplicable rise in last triennium of CEMACH report.
-Obesity in Pregnancy
Journal Review Articles worth looking at
BJA
2007
August: Carotid endarterectomy
September: Perioperative platelet Rx
December: Gabapentin
2008
February: Prone position
March: VAP
September: Perioperative management of pts with renal failure
Anaesthesia
2007
October/November: Interpleural block parts 1&2
December: Remifentanil
Previous SAQs done badly as highlighted in the Examiner's Report
- Preop assessment of a hypertensive patient (October 2007 SAQ paper)
- Management of twins (October 2007 SAQ paper)
- Air Embolus (April 2008 SAQ paper)
- Paediatric Fluid Balance (April 2008 SAQ paper)
- Neuromuscular Blocking Reversal + Sugammadex (April 2008 SAQ paper)
Other topics include issues of public interest and patient safety which were highlighted in the Examiner's report as being repeatedly done badly and therefore will continue to be represented in the examination, guidelines (including AAGBI, NICE, NPSA), and review articles from major journals.
-Awareness: continually remains in the public eye
-Healthcare-associated infections (VIP cannula scores/MRSA/C.Diff): huge at present also linked with recent publication by the aagbi on Infection in Anaesthesia
-CEMACH - easily repeated question
-Mental Capacity Act - has come into force in late 2007. This is the link I used previously, but for much more comprehensive coverage of both this and issues of Consent, EI has done a fantastic job putting togther some very simple explanations of tricky topics!
-LA toxicity +/- Intralipid use - it's going to come up eventually
-Malignant Hyperthermia treatment
-Blood Transfusion
-Perioperative Management of the Morbidly Obese Patient
-Prophylaxis against Infective Endocarditis: NICE March 2008
-Perioperative hypothermia: NICE April 2008
-Head Injury: NICE September 2007
-VAP: NICE August 2008
-CEPEX testing here
-POISE (Perioperative Ischaemic Evaluation) study: looks at beta-blocker use in non-cardiac surgery
-Amniotic Fluid Embolism: inexplicable rise in last triennium of CEMACH report.
-Obesity in Pregnancy
Journal Review Articles worth looking at
BJA
2007
August: Carotid endarterectomy
September: Perioperative platelet Rx
December: Gabapentin
2008
February: Prone position
March: VAP
September: Perioperative management of pts with renal failure
Anaesthesia
2007
October/November: Interpleural block parts 1&2
December: Remifentanil
The Written Paper
SAQs
For candidates sitting the exam for the first time, the SAQ section can seem the most daunting of the two. This style of exam has not been approached or attempted before (except in my case - wry laugh at onesself!). Adam has highlighted in his recent posting on Exam Intelligence the importance of layout of your SAQs. As you can see from his jpeg examples, it makes a huge difference to the examiner marking the paper. One little tactic is to try and put yourself in the examiner's shoes: you have 60 or 70 copies of the same question to mark, you're probably going to get a bit bored after a while - it's human nature. It must be intensely irritating to arrive at a question that you can't read, or is squashed against the far margin (or is irrelevant!). So, here is some SAQ advice:
- Learn to write nicely - make it larger and well spaced-out. Start practicing now - don't wait until the day.
- Be relevant; answer the question asked. It sounds obvious but you'd be surprised. You only get approximately 10-12 minutes to write the question (plus two-three minutes planning). Don't waste time on lengthy definitions/introductions if not asked for.
- Use diagrams - as mentioned in a previous posting, an accurately-labelled diagram may save you a lot of time and gain more marks than a block of prose.
- Get your timing right - this section of the exam is time-pressured. Work out your strategy of answering questions i.e. do you work through the paper sequentially making a question plan then answering the question, or do you make plans for all questions in the paper, then answer them? You must have a game-plan thought out.
- If you haven't already started, time your questions...strictly! You have to complete all 12 questions in 3 hours; that's 15 mins per question. Anyone who has done the exam before will tell you it is exhausting and they're right. To write solidly for 3 hours is difficult, both on your hand and on your mind. Like running a marathon, you need to train for it, and build up your stamina in answering these questions. Start by answering 4, then 6, then 8, then 12 questions in a row...timed!
MCQs
A word of warning, ignore these at your peril. There is a tendency to concentrate on the SAQ section, thinking that past experience in MCQs will see you through. This is the mistake I made and I paid for it with a 1+ and that is part of the reason why I have the privilege of doing this again. I probably can't offer much in the way of new advice on how to be successful with MCQs - everyone has quite extensive experience. Do as many MCQs as you can lay your hands on. The only difference this time around is that negative marking has been removed and consequently the pass mark will increase. You should probably be aiming to achieve approximately 80% i.e. average of 4/5 on each stem.
For candidates sitting the exam for the first time, the SAQ section can seem the most daunting of the two. This style of exam has not been approached or attempted before (except in my case - wry laugh at onesself!). Adam has highlighted in his recent posting on Exam Intelligence the importance of layout of your SAQs. As you can see from his jpeg examples, it makes a huge difference to the examiner marking the paper. One little tactic is to try and put yourself in the examiner's shoes: you have 60 or 70 copies of the same question to mark, you're probably going to get a bit bored after a while - it's human nature. It must be intensely irritating to arrive at a question that you can't read, or is squashed against the far margin (or is irrelevant!). So, here is some SAQ advice:
- Learn to write nicely - make it larger and well spaced-out. Start practicing now - don't wait until the day.
- Be relevant; answer the question asked. It sounds obvious but you'd be surprised. You only get approximately 10-12 minutes to write the question (plus two-three minutes planning). Don't waste time on lengthy definitions/introductions if not asked for.
- Use diagrams - as mentioned in a previous posting, an accurately-labelled diagram may save you a lot of time and gain more marks than a block of prose.
- Get your timing right - this section of the exam is time-pressured. Work out your strategy of answering questions i.e. do you work through the paper sequentially making a question plan then answering the question, or do you make plans for all questions in the paper, then answer them? You must have a game-plan thought out.
- If you haven't already started, time your questions...strictly! You have to complete all 12 questions in 3 hours; that's 15 mins per question. Anyone who has done the exam before will tell you it is exhausting and they're right. To write solidly for 3 hours is difficult, both on your hand and on your mind. Like running a marathon, you need to train for it, and build up your stamina in answering these questions. Start by answering 4, then 6, then 8, then 12 questions in a row...timed!
MCQs
A word of warning, ignore these at your peril. There is a tendency to concentrate on the SAQ section, thinking that past experience in MCQs will see you through. This is the mistake I made and I paid for it with a 1+ and that is part of the reason why I have the privilege of doing this again. I probably can't offer much in the way of new advice on how to be successful with MCQs - everyone has quite extensive experience. Do as many MCQs as you can lay your hands on. The only difference this time around is that negative marking has been removed and consequently the pass mark will increase. You should probably be aiming to achieve approximately 80% i.e. average of 4/5 on each stem.
Sunday, 14 September 2008
HCAI
At the beginning of August, I didn't know what HCAI stood for. I certainly do now: healthcare-associated infections. As mentioned previously, this is big business in the NHS. As usual, there are mountains of paperwork associated with this, including lots of webpages which, if you have loads of free time on your hands and not a lot to do, you could trawl through. However, we have exams, therefore we need a concise summary of what is important to us as anaesthetists/intensivists for the Final FRCA. Below is an account which summarises and provides links to important guidelines/publications:
Saving Lives - Clean Safe Care
- In a nutshell, the aim is to reduce HCAIs and provide safe, clean, reliable healthcare.
Important Publications
- Winning Ways (Chief Medical Officer, Dec 2003): strategy for reducing HCAIs in UK.
- Towards cleaner hospitals & lower rates of infection (DoH, July 2004) - 6 elements:
1) Being open with the public i.e. regular publication of infection data
2) Giving power to the patients e.g. cleanyourhands campaign.
***On September 2nd, the NPSA released a Patient Safety Alert 'Clean Hands Save Lives'. The four page document can be downloaded from here.***
3) A matron's charter - ten principles for delivering cleaner hospitals
4) Independent inspection to measure progress
5) Learning from the very best i.e. home & abroad
6) Harnessing the latest research & technology
-Saving Lives (June 2005): a delivery programme for acute hospitals to reduce HCAIs using Essential Steps to Safe, Clean Care e.g. reducing MRSA strategies, preventing inter-patient contamination, urinary catheter care, enteral feeding infection risk education.
- Also of relevance to anaesthetists/intensivists are: High Impact Interventions (or Care Bundles). Important ones include:
a) CVC care
b) Peripheral intravenous cannula care (also see later)
c) Care for ventilated patients
d) Reducing the risk of Clostridium.difficile
- Going Further Faster II (June 2008): applying the learning to reduce HCAI and improve cleanliness. A long document incorporating recent national guidelines/aims in infection control.
In my trust, there is a new policy which aims to ensure that all peripheral cannulae are sited in an aseptic manner. There is also routine use of Visual Infusion Phlebitis charts/scoring. Information can be found here and here.
Saving Lives - Clean Safe Care
- In a nutshell, the aim is to reduce HCAIs and provide safe, clean, reliable healthcare.
Important Publications
- Winning Ways (Chief Medical Officer, Dec 2003): strategy for reducing HCAIs in UK.
- Towards cleaner hospitals & lower rates of infection (DoH, July 2004) - 6 elements:
1) Being open with the public i.e. regular publication of infection data
2) Giving power to the patients e.g. cleanyourhands campaign.
***On September 2nd, the NPSA released a Patient Safety Alert 'Clean Hands Save Lives'. The four page document can be downloaded from here.***
3) A matron's charter - ten principles for delivering cleaner hospitals
4) Independent inspection to measure progress
5) Learning from the very best i.e. home & abroad
6) Harnessing the latest research & technology
-Saving Lives (June 2005): a delivery programme for acute hospitals to reduce HCAIs using Essential Steps to Safe, Clean Care e.g. reducing MRSA strategies, preventing inter-patient contamination, urinary catheter care, enteral feeding infection risk education.
- Also of relevance to anaesthetists/intensivists are: High Impact Interventions (or Care Bundles). Important ones include:
a) CVC care
b) Peripheral intravenous cannula care (also see later)
c) Care for ventilated patients
d) Reducing the risk of Clostridium.difficile
- Going Further Faster II (June 2008): applying the learning to reduce HCAI and improve cleanliness. A long document incorporating recent national guidelines/aims in infection control.
In my trust, there is a new policy which aims to ensure that all peripheral cannulae are sited in an aseptic manner. There is also routine use of Visual Infusion Phlebitis charts/scoring. Information can be found here and here.
AAGBI
The Association of Anaesthetists' updated guidelines on Blood Transfusion and the Anaesthetist in June 2008 are available now online. They are well worth a read and should be part of core knowledge both in clinical practice and for the forthcoming exam.
Guidelines from organisations such as the Association of Anaesthetists, as I have mentioned previously, provide excellent exam topics as they are current and relevant. In the interest of being thorough, the Association also published Standards of Monitoring in March 2007. Whilst this should be second nature to us as anaesthetists and, indeed, common sense, there are important clinical guidelines highlighted.
Guidelines from organisations such as the Association of Anaesthetists, as I have mentioned previously, provide excellent exam topics as they are current and relevant. In the interest of being thorough, the Association also published Standards of Monitoring in March 2007. Whilst this should be second nature to us as anaesthetists and, indeed, common sense, there are important clinical guidelines highlighted.
Wednesday, 10 September 2008
Spring Clean
As you may have noticed, there are a few extras added to the site. As I have been so utterly fed up with revision in the past day or two, I reverted to the ultimate in procrastination and found some fun stuff to put on the blog. I realise that for the majority of time, I hope I'm posting some useful information/links etc about hot topics. Some of my friends who read this blog tell me that it gives the impression that I'm constantly working extremely hard and am very well prepared. You'll be delighted to hear that in fact I am completely human and some days really struggle to open a book. Like today....!! So, I hope that this posting will bring some comfort to everyone who has crap days where the brain is resisting attempts to revise.
There is a live traffic feed on the bottom left margin to see where everyone is coming from and going to via this site - if you feel this is a infringement on your privacy, you are able to opt your browser out by clicking on the options button at the bottom of it. No-one gets any personal information from you - it's purely an interest thing for the geek in me!
Only 40 days to go until the written - chins up!
There is a live traffic feed on the bottom left margin to see where everyone is coming from and going to via this site - if you feel this is a infringement on your privacy, you are able to opt your browser out by clicking on the options button at the bottom of it. No-one gets any personal information from you - it's purely an interest thing for the geek in me!
Only 40 days to go until the written - chins up!
Friday, 5 September 2008
Make your life easy!
'A picture is worth a thousand words' (Fred R Barnard 1921)
The above quote can be applied to many parts of this exam, most specifically to anatomy. There will be an anatomy/regional technique SAQ and there will be an anatomy SOE. With that type of guarantee, one must be well prepared and learn thoroughly the anatomy syllabus. If you can produce a slick, well-labelled diagram, it looks impressive to the examiners and you will earn many more marks than trying to write a block of anatomical prose or talk through the roots of the lumbar plexus! I speak from experience, having 'come a cropper' in the anatomy section of my science viva (I will try to follow my own advice next time!).
My former exam buddy Dr B (FRCA) had a great method for anatomy and graph revision; he used a white board and continually drew and re-drew the diagrams, whilst talking to himself about what he was drawing as if explaining to the examiners. It then became second nature to reproduce what was required within seconds.
I used two textbooks for my revision: Anatomy for Anaesthetists & Concise Anatomy for Anaesthesia. I also used AnaesthesiaUK, Instant Anatomy, New York School of Regional Anesthesia, and Google Images. So what do you need to know? Well, basically all of the Primary syllabus but in a clinically-orientated manner. So, not just "Draw the brachial plexus" but "Describe with the use of a diagram which nerves are blocked with an interscalene block. Tell me how you would perform the block, and what are the contraindications/complications".
Below is a list of stuff you should know from head to toe - not definitive but should cover the majority of the syllabus:
Cerebral circulation
Cranial Nerves
The Eye: Clinical = blocks
Nerve supply to the face: Clinical = trigeminal neuralgia
Nose: it has been asked in the past!
Internal Jugular & Subclavian Vein: Clinical = cannulation
Cervical plexus and here: Clinical = superficial/deep cervical plexus blocks (+ GA vs RA for carotids)
Neck surface anatomy: Clinical = tracheostomy (+ surgical vs perc + cross-section @ C6)
Stellate ganglion: Clinical = block
Larynx and here: Clinical = LA/RA for awake fibreoptic intubation
Tracheobronchial tree: Clinical = one-lung anaesthesia/DLT
Pleural space: Clinical = intercostal N block/interpleural block/paravertebral block
Coronary circulation: Arterial & Venous
Autonomic Nervous System: so many questions!! ?Valsava manoeuvre
Coeliac plexus: Clinical = block
Lumbar plexus: Clinical = block (+ lumbar sympathetic block)
Sacral plexus
Sacrum: Clinical = Caudal anaesthesia (usually paediatric)
Femoral Triangle: Clinical = '3-in-1' blocks
Femoral Nerve: Clinical = as above
Sciatic Nerve: Clinical = blocks (different approaches)
Nerve supply to foot: Clinical = ankle block
The above quote can be applied to many parts of this exam, most specifically to anatomy. There will be an anatomy/regional technique SAQ and there will be an anatomy SOE. With that type of guarantee, one must be well prepared and learn thoroughly the anatomy syllabus. If you can produce a slick, well-labelled diagram, it looks impressive to the examiners and you will earn many more marks than trying to write a block of anatomical prose or talk through the roots of the lumbar plexus! I speak from experience, having 'come a cropper' in the anatomy section of my science viva (I will try to follow my own advice next time!).
My former exam buddy Dr B (FRCA) had a great method for anatomy and graph revision; he used a white board and continually drew and re-drew the diagrams, whilst talking to himself about what he was drawing as if explaining to the examiners. It then became second nature to reproduce what was required within seconds.
I used two textbooks for my revision: Anatomy for Anaesthetists & Concise Anatomy for Anaesthesia. I also used AnaesthesiaUK, Instant Anatomy, New York School of Regional Anesthesia, and Google Images. So what do you need to know? Well, basically all of the Primary syllabus but in a clinically-orientated manner. So, not just "Draw the brachial plexus" but "Describe with the use of a diagram which nerves are blocked with an interscalene block. Tell me how you would perform the block, and what are the contraindications/complications".
Below is a list of stuff you should know from head to toe - not definitive but should cover the majority of the syllabus:
Cerebral circulation
Cranial Nerves
The Eye: Clinical = blocks
Nerve supply to the face: Clinical = trigeminal neuralgia
Nose: it has been asked in the past!
Internal Jugular & Subclavian Vein: Clinical = cannulation
Cervical plexus and here: Clinical = superficial/deep cervical plexus blocks (+ GA vs RA for carotids)
Neck surface anatomy: Clinical = tracheostomy (+ surgical vs perc + cross-section @ C6)
Stellate ganglion: Clinical = block
Brachial plexus: Clinical = block
Axilla
Ulnar/radial/median nerves: Clinical = blocks (from BP to wrist)
Larynx and here: Clinical = LA/RA for awake fibreoptic intubation
Tracheobronchial tree: Clinical = one-lung anaesthesia/DLT
Pleural space: Clinical = intercostal N block/interpleural block/paravertebral block
Coronary circulation: Arterial & Venous
Epidural space: Clinical = epidural anaesthesia
Subarachnoid space: Clinical = spinal anaesthesia
Vertebrae: Clinical = as above/vertebral space
Spinal cord and here: Clinical = arterial blood supply
Autonomic Nervous System: so many questions!! ?Valsava manoeuvre
Coeliac plexus: Clinical = block
Lumbar plexus: Clinical = block (+ lumbar sympathetic block)
Sacral plexus
Sacrum: Clinical = Caudal anaesthesia (usually paediatric)
Femoral Triangle: Clinical = '3-in-1' blocks
Femoral Nerve: Clinical = as above
Sciatic Nerve: Clinical = blocks (different approaches)
Nerve supply to foot: Clinical = ankle block
Saturday, 30 August 2008
It's hot out there...
A quick posting to draw your attention to the recently published NICE guidelines (August 2008) on:
Technical patient safety solutions for ventilator-associated pneumonia in adults
There was an SAQ in May 2005 on VAP, so perhaps time for a revisit??
These will be the last set of NICE guidelines published before the exam setting mid-September.
Anyone else finding the hot weather difficult to revise in?? ;)
Technical patient safety solutions for ventilator-associated pneumonia in adults
There was an SAQ in May 2005 on VAP, so perhaps time for a revisit??
These will be the last set of NICE guidelines published before the exam setting mid-September.
Anyone else finding the hot weather difficult to revise in?? ;)
Tuesday, 26 August 2008
STOP PRESS!!
The word on the street is all about reducing Hospital Acquired Infections. Anyone who has attended a hospital induction this month will have been bombarded by both the corporate, clinical, and departmental teams regarding the importance of limiting infections. Never before in my career have I witnessed such emphasis on one particular area. Heck, I even had to attend mandatory training on taking blood cultures and inserting cannulae (and have the certificate to prove it - so proud!).
Why is this huge? Apart from the obvious continual negative media attention reveived with daily uproar (and obviously the detrimental effect on patients - how could I forget to mention this?!), this is big bucks for the hospitals. There will be financial penalties for those Trusts failing to comply and suffering high HAI rates.
How does it affect us? Well, apart from changing our clinical practice, it may save us £690. Why? Because (Yes, I know I've started a sentence with 'because'; pedants!) of it's extreme topical nature, it could be a Short Answer Question, or even appear in the Structured Oral section of the exam. I refer you to Exam Intelligence who has already alerted readers of his blog as to the potential of this line of questioning. He outlines what the Royal College have said - we need to be aware of topical issues, and none is hotter than this at the moment. More information can be found on the Clean, Safe Care NHS website.
This is emphasised this month, as if by magic, by our beloved Association of Anaesthetists in the publication of updated guidelines on Infection Control in Anaesthesia (September 2008 edition of Anaesthesia p.1027). This is a must-read as it is concise, topical, and most importantly, relevant to anaesthesia.
Why is this huge? Apart from the obvious continual negative media attention reveived with daily uproar (and obviously the detrimental effect on patients - how could I forget to mention this?!), this is big bucks for the hospitals. There will be financial penalties for those Trusts failing to comply and suffering high HAI rates.
How does it affect us? Well, apart from changing our clinical practice, it may save us £690. Why? Because (Yes, I know I've started a sentence with 'because'; pedants!) of it's extreme topical nature, it could be a Short Answer Question, or even appear in the Structured Oral section of the exam. I refer you to Exam Intelligence who has already alerted readers of his blog as to the potential of this line of questioning. He outlines what the Royal College have said - we need to be aware of topical issues, and none is hotter than this at the moment. More information can be found on the Clean, Safe Care NHS website.
This is emphasised this month, as if by magic, by our beloved Association of Anaesthetists in the publication of updated guidelines on Infection Control in Anaesthesia (September 2008 edition of Anaesthesia p.1027). This is a must-read as it is concise, topical, and most importantly, relevant to anaesthesia.
Thursday, 21 August 2008
ICU-itis
My ICU shifts recently have been so hectic and busy that I've not had a chance to participate in the sport of Academia at Olympic levels recently! I have started ploughing through Elfituri & Arthur's MCQ book - with a resounding 76% in the first paper - I was quite pleased at that, although I still seem to make the same mistakes as I did the last time I attempted the paper. I had also worked my way through the October 2007 SAQ paper, and will share some more ideas about this paper later in September.
Although the workload has been heavy, I've had some opportunities to put some Final's knowledge to good use. I encountered a chap on the medical ward last night whose K+ was 8.9 (and still alive) - even post-treatment, his broad complex ECG made for a sphincter-tightening journey to ICU!! The question on life-threatening hyperkalaemia (?October 2007) seemed quite appropriate all of a sudden. I also brightened up my evening with a failed intubation on ICU (unexpected Grade 4 laryngoscopy: Consultant-confirmed. They usually subtract 1 from what the trainee makes the grade!!) - thank you to Archie Brain for the provision of the LMA.
I've got some days off coming up soon, and hope to summarise a few more topics related to the exam. If anyone has any topics which they feel are relevant, or not covered well in textbooks - please share by leaving some comments, or emailing me (jrs970@yahoo.co.uk)
Although the workload has been heavy, I've had some opportunities to put some Final's knowledge to good use. I encountered a chap on the medical ward last night whose K+ was 8.9 (and still alive) - even post-treatment, his broad complex ECG made for a sphincter-tightening journey to ICU!! The question on life-threatening hyperkalaemia (?October 2007) seemed quite appropriate all of a sudden. I also brightened up my evening with a failed intubation on ICU (unexpected Grade 4 laryngoscopy: Consultant-confirmed. They usually subtract 1 from what the trainee makes the grade!!) - thank you to Archie Brain for the provision of the LMA.
I've got some days off coming up soon, and hope to summarise a few more topics related to the exam. If anyone has any topics which they feel are relevant, or not covered well in textbooks - please share by leaving some comments, or emailing me (jrs970@yahoo.co.uk)
Wednesday, 13 August 2008
Down Under...
As well as roaring past the 2500 hits mark, the blog has been recommended on an Australian website: Anaesthesiacases
They write: "James Shorthouse’s Blogspot!! This is great reading: the keeping of a diary in the approach to the final FRCA exam. Good for the final exam candidate but also for the consultant browsing on a range of clinical topics". I'm thrilled to have received some international recognition!!
Back to the job in hand: having just finished a stupendous ten day stretch in ICU, I've been trying to catch up with some revision. I've just filled out my application form for the exam, together with a(nother) cheque for £690. Remember that the closing date is September 9th.
I've been through and repeated the SAQ paper I did in April this year, specifically concentrating on questions which were done badly by candidates i.e. air embolism, paediatric fluid resuscitation, and neuromuscular blockade reversal. All questions were done to a strict 10-11 minute time-limit, and I reviewed my answers and annotated them for further reference.
I have also completed the 270 MCQs in the new RCOA guide to the Final FRCA, in 3 batches of 90. Pleasingly, I managed to score 77%, 78%, and 79% respectively (aiming for 80% passmark). Bear in mind, some of these questions I've done before. On a negative turn of events, I attempted some Q-Base 5 questions on the computer. Firstly, I think in future I will do these Q-Base MCQs on paper as the CD-ROM only do negative marking. Secondly, they are in batches of 60, so you get out of sync with the papers - I believe we need to be practicing 90 MCQs at a time. Thirdly (& less importantly), there's something I really don't like about Q-Base questions i.e. they're hard and I only got 36% this time round! Just like last time, I always end up swearing at the computer during Q-Base!!!
They write: "James Shorthouse’s Blogspot!! This is great reading: the keeping of a diary in the approach to the final FRCA exam. Good for the final exam candidate but also for the consultant browsing on a range of clinical topics". I'm thrilled to have received some international recognition!!
Back to the job in hand: having just finished a stupendous ten day stretch in ICU, I've been trying to catch up with some revision. I've just filled out my application form for the exam, together with a(nother) cheque for £690. Remember that the closing date is September 9th.
I've been through and repeated the SAQ paper I did in April this year, specifically concentrating on questions which were done badly by candidates i.e. air embolism, paediatric fluid resuscitation, and neuromuscular blockade reversal. All questions were done to a strict 10-11 minute time-limit, and I reviewed my answers and annotated them for further reference.
I have also completed the 270 MCQs in the new RCOA guide to the Final FRCA, in 3 batches of 90. Pleasingly, I managed to score 77%, 78%, and 79% respectively (aiming for 80% passmark). Bear in mind, some of these questions I've done before. On a negative turn of events, I attempted some Q-Base 5 questions on the computer. Firstly, I think in future I will do these Q-Base MCQs on paper as the CD-ROM only do negative marking. Secondly, they are in batches of 60, so you get out of sync with the papers - I believe we need to be practicing 90 MCQs at a time. Thirdly (& less importantly), there's something I really don't like about Q-Base questions i.e. they're hard and I only got 36% this time round! Just like last time, I always end up swearing at the computer during Q-Base!!!
Tuesday, 29 July 2008
Sugamma.....something or other
The only reason I had heard of this prior to the SAQs in April was because one of my previous bosses, who I did regular lists with as an SHO, was fascinated by it and would discuss it regularly - amazing to think that even a couple of years later those 'discussions' would be useful to me! So what's all the fuss about?

Codenames
- Org 25969
- Modified γ-cyclodextrin
Structure
- Lipophilic core and hydrophilic periphery enabling the molecule to engulf and bind lipophilic molecules while maintaining aqueous solubility (8 negatively-charged thio ether extensions are situated at the 6th carbon position of each ring, thus extending the cavity size allowing greater encapsulation of the rocuronium molecule).

Mechanism of action
Mechanism of action
- The first selective relaxant binding agent - it forms very tight water-soluble complexes at a 1:1 ratio with aminosteroidal neuromuscular blocking drugs e.g. rocuronium, preventing them from binding to the ACh molecule and exerting muscular relaxation.
Uses
Uses
- Reversal of profound neuromuscular blockade without the need to inhibit acetylcholinesterase i.e. eliminating the autonomic/CVS effects of the more traditional acetylcholinesterase inhibitors(neostigmine) and the concomitant antimuscarinics (glycopyrrolate) that must be also administered. (Phase 3 trials)
- Elimination of the incomplete reversal experienced with use of traditional acetylcholinesterase inhibitors.
- Also, the rapid onset (and now reversal by Sugammadex) of action of rocuronium could make it a safer alternative to suxamethonium in rapid sequence inductions.
Pharmacodynamics/Pharmacokinetics
- No effects on other receptor systems in body i.e. biologically inactive
- Does not bind to plasma protein
- No renal excretion
- No renal excretion
Monday, 28 July 2008
Is it Pimms o'Clock yet?
Exam Intelligence has a spanking sparkly new website up and running now - if you haven't already checked it out, it's definitely worth bookmarking for the breadth and sheer effort put in by Adam in providing valuable information to pass this exam.
My website skills are minimal but what I will continue to try and achieve is a regular update of both my revision progress (poor at present - anyone else feeling a bit lethargic in the hot weather?) and useful information, links etc.
Someone emailed me recently asking for advice about SAQs. RCOA have just produced their report on the April SAQ paper. This, in my opinion, is a great revision aid alone. It gives a unique insight into what the examiners expect from the SAQ answers.
Here are some thoughts:
-"Despite the questions being printed in the answer books, a small number of candidates failed to
answer all the questions." You will fail if you don't answer all the questions - that is expensive and time-consuming!!
-"Questions: 3 (air embolus), 4 (paediatric fluid balance) and 7 (neuromuscular blocking reversal) caused the most problems to candidates" Something to think about for next time maybe?
-"Question1 (paravertebral space) was generally well done but few candidates did a really good
anatomy section. The diagrams were especially poor – examiners assumed this was due to lack of knowledge." A diagram (even simple but well labelled) will get you a lot more marks and take less time than a block of prose.
-"Whilst the web sites related to the FRCA are mostly useful and enjoyable, there are occasional
moments when it is disappointing to see unhelpful advice being offered. This particularly relates to generic answers and, for example, it is rarely the case that a whole ‘pre, per and post op’ structure would facilitate a good answer on the SAQ paper.... It cannot be emphasised enough that the answer provided to the examiners is less than a page and is focused completely to the question." This is a fair point: as my experience of writing SAQs has grown, I have realised that there is no time for a complete generic answer. Whilst it can give you structure, usually in a viva, in the SAQs the answer has to be much more specific. In theory, you should be able to pass the question writing between one to two A4 sides of concise and relevant bullet points/labelled-diagrams. Paragraphs are unsightly, difficult to mark, and a waste of time that you do not have.
My website skills are minimal but what I will continue to try and achieve is a regular update of both my revision progress (poor at present - anyone else feeling a bit lethargic in the hot weather?) and useful information, links etc.
Someone emailed me recently asking for advice about SAQs. RCOA have just produced their report on the April SAQ paper. This, in my opinion, is a great revision aid alone. It gives a unique insight into what the examiners expect from the SAQ answers.
Here are some thoughts:
-"Despite the questions being printed in the answer books, a small number of candidates failed to
answer all the questions." You will fail if you don't answer all the questions - that is expensive and time-consuming!!
-"Questions: 3 (air embolus), 4 (paediatric fluid balance) and 7 (neuromuscular blocking reversal) caused the most problems to candidates" Something to think about for next time maybe?
-"Question1 (paravertebral space) was generally well done but few candidates did a really good
anatomy section. The diagrams were especially poor – examiners assumed this was due to lack of knowledge." A diagram (even simple but well labelled) will get you a lot more marks and take less time than a block of prose.
-"Whilst the web sites related to the FRCA are mostly useful and enjoyable, there are occasional
moments when it is disappointing to see unhelpful advice being offered. This particularly relates to generic answers and, for example, it is rarely the case that a whole ‘pre, per and post op’ structure would facilitate a good answer on the SAQ paper.... It cannot be emphasised enough that the answer provided to the examiners is less than a page and is focused completely to the question." This is a fair point: as my experience of writing SAQs has grown, I have realised that there is no time for a complete generic answer. Whilst it can give you structure, usually in a viva, in the SAQs the answer has to be much more specific. In theory, you should be able to pass the question writing between one to two A4 sides of concise and relevant bullet points/labelled-diagrams. Paragraphs are unsightly, difficult to mark, and a waste of time that you do not have.
Saturday, 19 July 2008
Out of the blocks...True or False?
Since adding a counter to the website approximately two weeks ago, over 1000 people have had a look - many thanks. Feel free to leave (constructive) comments, and if there are any suggestions please either comment or email me: jrs970@yahoo.co.uk
I started work again yesterday with great difficulty and attempted upsurges in motivation. Actually quite an encouraging start: I began with the MCQs from the new edition college book, some of which I recognised from previously, and some which were new. It's a different ball game with MCQs from now on without the negative marking, as this takes the dilemma about leaving questions unanswered out of the game. All questions should be answered as there is nothing to lose, and the college is recommending 80% as a passmark (which is probably the equivalent of approx. 60% for the negatively marked paper). I got 77% on the first 90 questions - don't be too alarmed as I have done the damn exam before so hopefully would have retained some knowledge. The last time I started MCQs, I was getting dreadfully embarassing marks e.g. 20-30%!! My advice would be: do not underestimate this part of the exam - it is where I came unstuck at my peril. Practice practice practice.
It is also worth (if not already done so) thinking about courses. Not for everyone, granted, but they do focus the mind somewhat (and it's a weekend/week off work too!). My experience is entirely with the Mersey courses. I can't recommend the Booker Course highly enough for the experience, practice, timing, and lectures on SAQs -it really whips you into shape! There are also various weekends/weeks for SAQs/MCQs, and SOEs once you hopefully get there.
Other courses available can be found at Anaesthesia UK.
I started work again yesterday with great difficulty and attempted upsurges in motivation. Actually quite an encouraging start: I began with the MCQs from the new edition college book, some of which I recognised from previously, and some which were new. It's a different ball game with MCQs from now on without the negative marking, as this takes the dilemma about leaving questions unanswered out of the game. All questions should be answered as there is nothing to lose, and the college is recommending 80% as a passmark (which is probably the equivalent of approx. 60% for the negatively marked paper). I got 77% on the first 90 questions - don't be too alarmed as I have done the damn exam before so hopefully would have retained some knowledge. The last time I started MCQs, I was getting dreadfully embarassing marks e.g. 20-30%!! My advice would be: do not underestimate this part of the exam - it is where I came unstuck at my peril. Practice practice practice.
It is also worth (if not already done so) thinking about courses. Not for everyone, granted, but they do focus the mind somewhat (and it's a weekend/week off work too!). My experience is entirely with the Mersey courses. I can't recommend the Booker Course highly enough for the experience, practice, timing, and lectures on SAQs -it really whips you into shape! There are also various weekends/weeks for SAQs/MCQs, and SOEs once you hopefully get there.
Other courses available can be found at Anaesthesia UK.
Tuesday, 15 July 2008
Read the press.....
Guidelines and national publications for two years previously are much beloved of this exam. Common places to look include:
The Association of Anaesthetists (2007-8)
-LA toxicity +/- Intralipid use
-Malignant Hyperthermia treatment
-Perioperative Management of the Morbidly Obese Patient - THIS IS FAIR GAME FOR THIS YEAR!!
-Standards of monitoring during anaesthesia & recovery
-Blood Transfusion & the Anaesthetist (recent publication: I will summarise very soon)
NICE (2007-8)
-Venous Thromboembolism: April 2007
-Acutely Ill patients in hospital: July 2007
-Head Injury: September 2007
-Intrapartum Care: September 2007
-Ultrasound Guidance in locating the Epidural Space: January 2008
-Prophylaxis against Infective Endocarditis: March 2008
-Perioperative hypothermia: April 2008
-Technical solutions for VAP in adults: August 2008
NPSA
Reducing the risk of hyponatraemia when administering intravenous infusions to children
-Since 2000, there have been four child deaths following neurological injury from hospital-acquired hyponatraemia reported in the UK.
Recommendations
-Remove 0.18% NaCl with glucose 4% from stocks & general use in areas treating children.
-Produce local clinical guidelines for the fluid management of paediatric patients.
-Provide adequate supervision and training for all staff involced in the prescribing, monitoring, and administering of IV fluids for children.
-Review & improve design of existing drug prescription/fluid balance charts.
-Promote reporting of hospital-acquired hyponatraemia incidents
Resuscitation: intravascular volume depletion should be managed with 0.9% NaCl boluses
Deficit: estimate fluid deficit & replace as 0.9% NaCl with 5% dextrose or 0.9% NaCl over a minimum of 24hrs
Maintenance: do not use 0.18% NaCl with glucose 4%
The majority of children may be managed with 0.45% NaCl with 5% glucose (or 2.5% glucose)
CEMACH (report summarised in previous blog posting)
The Association of Anaesthetists (2007-8)
-LA toxicity +/- Intralipid use
-Malignant Hyperthermia treatment
-Perioperative Management of the Morbidly Obese Patient - THIS IS FAIR GAME FOR THIS YEAR!!
-Standards of monitoring during anaesthesia & recovery
-Blood Transfusion & the Anaesthetist (recent publication: I will summarise very soon)
NICE (2007-8)
-Venous Thromboembolism: April 2007
-Acutely Ill patients in hospital: July 2007
-Head Injury: September 2007
-Intrapartum Care: September 2007
-Ultrasound Guidance in locating the Epidural Space: January 2008
-Prophylaxis against Infective Endocarditis: March 2008
-Perioperative hypothermia: April 2008
-Technical solutions for VAP in adults: August 2008
NPSA
Reducing the risk of hyponatraemia when administering intravenous infusions to children
-Since 2000, there have been four child deaths following neurological injury from hospital-acquired hyponatraemia reported in the UK.
Recommendations
-Remove 0.18% NaCl with glucose 4% from stocks & general use in areas treating children.
-Produce local clinical guidelines for the fluid management of paediatric patients.
-Provide adequate supervision and training for all staff involced in the prescribing, monitoring, and administering of IV fluids for children.
-Review & improve design of existing drug prescription/fluid balance charts.
-Promote reporting of hospital-acquired hyponatraemia incidents
Resuscitation: intravascular volume depletion should be managed with 0.9% NaCl boluses
Deficit: estimate fluid deficit & replace as 0.9% NaCl with 5% dextrose or 0.9% NaCl over a minimum of 24hrs
Maintenance: do not use 0.18% NaCl with glucose 4%
The majority of children may be managed with 0.45% NaCl with 5% glucose (or 2.5% glucose)
CEMACH (report summarised in previous blog posting)
Journals
Thanks to everyone who is visiting the site - I now have a little counter to the left to get an idea of readership. It first went up about two weeks ago, and I've had nearly 800 views (thanks to Mum for all of them!).
As I have mentioned previously, the review articles in our journals (BJA & Anaesthesia) provide some ideal SAQ/SOE hot topics for the exam. It is important to recognise that there are some subjects much more likely to appear in an exam setting than others e.g. remifentanil as apposed to mitochondrial disorders! I estimate that approximately a year and a half's worth of articles are covered, so everything from April 2007 - September 2008. I have made what I consider to be exam topics in bold type:
BJA: here & here
2007
April: Blood flow & ventilation in the lung / percussion pacing
May: CA stents in non-cardiac surgery
June: Diastolic heart failure
July: Neuro ++! The whole post-grad issue is neuroanaesthesia/NICU reviews
August: Carotid endarterectomy
September: Perioperative platelet Rx
October: Sciatica & epidural injections / contrast-induced nephropathy
November: Cardioprotection with remote ischaemic preconditioning
December: Gabapentin
2008
January: Sedation & Regional anaesthesia
February: Prone position / epidural analgesia vs periph NB for knee surgery
March: Statins & Sepsis / VAP
April: Mitochondrial disorders
May: Perioperative anaemia management
June: Opioids & respiratory control
July: Its all about Pain! A whole postgraduate educational issue! Read the reviews.
August: Physiological effects of hyperchloraemia and acidosis + Acupuncture for post-operative pain
September: Perioperative management of pts with renal failure
Anaesthesia here and here
2007
April: Temp. epicardial pacing part 2
May: Systemic complications post-head injury
July: Propofol-infusion syndrome
October: Interpleural block part 1
November: Interpleural block part 2 / new thrombotic agents & neuraxial anaesthesia for major orthopaedic surgery
December: Remifentanil
2008
January: Oesophageal Doppler in abdominal surgery / Statins for non-cardiac surgery part1
February: Statins for non-cardiac surgery part 2 / cardiac output monitoring
March: Helium & Xenon / Metabolic acidosis in the critically ill Part 1
April: Metabolic Acidosis in the critically ill Part 2
June: IV contrast
July: Intubation aids
As I have mentioned previously, the review articles in our journals (BJA & Anaesthesia) provide some ideal SAQ/SOE hot topics for the exam. It is important to recognise that there are some subjects much more likely to appear in an exam setting than others e.g. remifentanil as apposed to mitochondrial disorders! I estimate that approximately a year and a half's worth of articles are covered, so everything from April 2007 - September 2008. I have made what I consider to be exam topics in bold type:
BJA: here & here
2007
April: Blood flow & ventilation in the lung / percussion pacing
May: CA stents in non-cardiac surgery
June: Diastolic heart failure
July: Neuro ++! The whole post-grad issue is neuroanaesthesia/NICU reviews
August: Carotid endarterectomy
September: Perioperative platelet Rx
October: Sciatica & epidural injections / contrast-induced nephropathy
November: Cardioprotection with remote ischaemic preconditioning
December: Gabapentin
2008
January: Sedation & Regional anaesthesia
February: Prone position / epidural analgesia vs periph NB for knee surgery
March: Statins & Sepsis / VAP
April: Mitochondrial disorders
May: Perioperative anaemia management
June: Opioids & respiratory control
July: Its all about Pain! A whole postgraduate educational issue! Read the reviews.
August: Physiological effects of hyperchloraemia and acidosis + Acupuncture for post-operative pain
September: Perioperative management of pts with renal failure
Anaesthesia here and here
2007
April: Temp. epicardial pacing part 2
May: Systemic complications post-head injury
July: Propofol-infusion syndrome
October: Interpleural block part 1
November: Interpleural block part 2 / new thrombotic agents & neuraxial anaesthesia for major orthopaedic surgery
December: Remifentanil
2008
January: Oesophageal Doppler in abdominal surgery / Statins for non-cardiac surgery part1
February: Statins for non-cardiac surgery part 2 / cardiac output monitoring
March: Helium & Xenon / Metabolic acidosis in the critically ill Part 1
April: Metabolic Acidosis in the critically ill Part 2
June: IV contrast
July: Intubation aids
Tuesday, 8 July 2008
Little People
I'm still taking a break from work, probably for another couple of weeks before I start up again. I will continue to post some useful stuff that I found helpful the last time.
Here is a list of useful paediatric formulae etc
Sedation
Midazolam: 2-8mcg/kg/min
Morphine: 20-40mcg/kg/min
CPR: 15:2
DC cardioversion: 4J/kg
Glucose: 2-4mls/kg of 10% dextrose
Here is a list of useful paediatric formulae etc
Neonate
-1st 44wks postconceptual age
-TV = 7ml/kg
-CO = 200ml/kg/min
-Blood vol = 90ml/kg
Infant
-Up to 12 months
-Weight = (Age in months + 9)/2
-TV = 6-8ml/kg
-Blood vol = 85ml/kg
Child
-1-12 years
-Weight = (Age + 4) x 2
-Blood vol = 80ml/kg
-Mean SBP = 90 + (age x 2)
Fluids
-Maintenance: 4ml/kg/hr for 1st 10kg. 2ml/kg/hr for 2nd 10kg. 1ml/kg/hr for subsequent kgs
-0.9% saline/Hartmanns + dextrose if required
-Fluid Bolus: 20ml/kg
Equipment
LMA size
1 (0-5kg)-cuff 2-5mls.
1.5 (5-10kg)-5-7mls.
2 (10-20kg)-7-10mls.
2.5 (20-30kg)-12-14mls.
3 (>30kg)-15-20mls.
-Uncuffed until 8-10yrs
ETT size
>2kg = 2.5mm
2-4kg = 3.0mm
Term neonate = 3.5mm
3 months-1yr = 4.0mm
>2yrs = (Age/4) + 4 (some books say + 4.5)
ETT length
oral (age/2) + 12
nasal (age/2) + 15
-TV= 10mls/kg
-PCV 18-20cmH2O/RR 16-24
-Min FGF 3L
-Insp press = 18-20cmH2O
-RR = 16-24
Fasting
-Clear fluid 2hrs
-Breast Milk/Formula 4hrs (<12months)
-Solids (& milk) 6hrs
Drugs
-EMLA: 2.5% lignocaine & 2.5% prilocaine (45mins)
-Ametop: 4% amethocaine gel (30mins)
-Midazolam 0.1-0.2mg/kg (PO 0.5mg/kg)
-(Flumazenil 5µg/kg incr to 40µg/kg)
-Temazepam 0.5-1mg/kg
-Fentanyl 1-5µg/kg (up to 25µg/kg: cardiac)
-Propofol 2-5mg/kg
-Thiopentone 4-6mg/kg
-(Etomidate 0.3mg/kg (0.1-0.4))
-Ketamine 2mg/kg (5-7mg/kg IM)
-Suxamethonium 2mg/kg
-Atropine 10µg/kg (20µg/kg IM)
-Adrenaline 0.1ml/kg 1:10000 (10µg/kg)
-Atracurium 0.5mg/kg
-Rocuronium 0.6mg/kg
-Vecuronium 0.1mg/kg
-Neo/Glyco 0.02ml/kg
(dilute 1ml w. 4ml saline give 0.1ml/kg).
-Morphine 0.1-0.2mg/kg 4hrly
-Oramorph 0.4mg/kg
(Naloxone 5-10µg/kg)
-Paracetamol 20-30mg/kg loading then 15mg/kg qds
-Diclofenac 1mg/kg tds (max 3mg/kg/day)
-Ibuprofen 5-10mg/kg tds
-Codeine phos 1mg/kg qds
-Cefuroxime 20-30mg/kg tds
-Metronidazole 7.5mg/kg
-Augmentin 25-50mg/kg qds
-Erythromycin 10-25mg/kg
-Cyclizine 1mg/kg
-Dexamethasone 0.15mg/kg
Ondansetron >2yrs 0.1mg/kg
Armitage regime
-0.25% bupivacaine
-Lumbosacral: 0.5ml/kg
-Thoracolumbar: 1ml.kg
-Midthoracic: 1.25ml/kg
Add
-clonidine 1µg/kg,
-diamorphine 30µg/kg,
-PF ketamine 0.5mg/kg,
-PF morphine 50µg/kg
-Wound infiltration 1ml/kg 0.25% bupivacaine
Epidurals
Loading dose:
-0.75ml/kg(lumbar) or 0.5ml/kg(thoracic) of 0.25% bupivacaine
Infusion:
-60ml of 0.125% bupivacaine + 2µg/ml fentanyl
Sedation
Midazolam: 2-8mcg/kg/min
Morphine: 20-40mcg/kg/min
CPR: 15:2
DC cardioversion: 4J/kg
Glucose: 2-4mls/kg of 10% dextrose
Friday, 4 July 2008
For the mothers
I know it came up in the April 2008 SAQs, but it's still a hot topic so here it is again:
CEMACH 2003-2005 Summary
Definition
- Confidential Enquiries into Maternal Deaths.
- The longest running "Gold Standard" audit in the world. First Report covered 1952-54
- Triennial report published by DOH looking into all maternal deaths in UK
- Changed title from “Why Mothers Die” to “Saving Mothers’ Lives”.
- All maternal deaths: 14 per 100000 maternities (no statistically significant change).
- Direct maternal mortality: slight rise (not statistically significant).
Causes of death:
- Direct: deaths of women while pregnant or within 42 days of termination of pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not accidental or incidental causes.
- Indirect: deaths resulting from previous existing disease, or disease that developed during pregnancy and which was not due to direct obstetric causes, but which was aggravated by the physiological effects of pregnancy.
- Late: deaths occurring between 42 days and one year after the end of pregnancy
Risk Factors contributing to maternal death
(Essentially the same as the lack of decline of maternal mortality)
- Lack of preconception care i.e counselling & support especially for serious physical/mental comorbidities, obesity, assisted reproduction/fertility, and identification of vulnerable/high risk mothers.
- Lack of access to antenatal care
- Migrants (poorer overall health, no medical review, genital mutilation)
- Increasing age of mothers
- Increasing incidence of obese mothers
- Increasing incidence of comorbidities e.g. DM/CVS disease
- Poor lifestyle e.g. smoking/drinking/drugs
Commonest direct causes of maternal death
1) Thromboembolism (again)
=2) Pre-eclampsia/sepsis
4) Amniotic fluid embolism
=5) Haemorrhage/early pregnancy
- Increased numbers of: pre-eclampsia, genital tract sepsis/trauma + inexplicable rise in amniotic fluid embolism.
- Decreased haemorrhage/early pregnancy/ectopic.
- Nil of above: statistically significant.
Commonest indirect cause of maternal death
- Cardiac disease (less healthy diets, smoking, alcohol and the growing epidemic of obesity).
Anaesthetics
- 150 cases reviewed: direct or indirect cause of death also having anaesthetic
Direct anaesthetic deaths:
- 6 deaths – (4.5%) 0.28 per 100000 maternities. Same as previous triennium.
- All but one: Caucasian.
- 4/6: obese (2 were morbidly obese: BMI > 35)
Cases
1) Post-op bronchospasm & resp failure: obese asthmatic lady – failed reintubation during recovery post laparascopic surgery for ectopic pregnancy. Irreversible cardiac arrest.
2) Obese lady, early pregnancy, trainee anaesthetist. High-dose opiate given prior to extubation. In recovery developed respiratory difficulties. Inadequate ventilation, bradycardia, cardiac arrest.
3) Morbidly obese asthmatic lady, elective LSCS, spinal anaesthesia. Post-op agitation and SOB. Fatal cardiac arrest on post-op ward with inadequate resuscitation equipment.
4) Low-dose infusion epidural during labour & forceps delivery. PPH + IVI + syntocinon infusions. Grand mal convulsion + VF arrest – unable to resuscitate. Given 150mls 0.1% bupivacaine IV.
5) Lady with pectus excavatum in mid-pregnancy: â foetal movements, fulminant PET, & HELLP. Hypertensive, hyperreflexic, oliguric, & abnormal LFTs – given labetalol, Mg, & hydralazine. For urgent LSCS: RIJ cannulation unsuccessful but subclavian cannulation successful on the second attempt. Cardiac arrest shortly afterwards – large right haemothorax.
6) Obese woman with longstanding renal problems requiring nephrectomy. Had premature labour and delivery. A few weeks later, she was admitted with fever, loin pain, and ileofemoral venous thrombosis. Planned for drainage of septic focus from remaining kidney under U/S guidance. Pt refused LA and suffered an irreversible cardiac arrest during GA.
Indirect Anaesthetic Deaths
-Further 31 cases where poor perioperative anaesthetic management may have contributed to outcome
- Failure to recognise serious illness
- Poor management of haemorrhage (including syntocinon use): Less than optimum anaesthetic management contributed to many of the 17 maternal deaths from haemorrhage (12 died from PPH).
- Sepsis: Poor anaesthetic management/resuscitation was thought to have contributed to 10 maternal deaths from sepsis (usually failure to appreciate seriousness of maternal condition).
- Pre-eclampsia/eclampsia: 4 women died in relation to poor anaesthetic management (usually related to poor control of systolic blood pressure at time of LSCS/post-operatively)
- Management of obese pregnant women
- Quality of in-house hospital Trust enquiries into serious untoward incidents including maternal deaths: some reports of internal hospital enquiries sent to CEMACH were lacking in insight, improperly conducted, did not include clinicians from relevant specialties, or included clinicians involved directly with the maternal death (potential bias).
CEMACH 2003-2005 Summary
Definition
- Confidential Enquiries into Maternal Deaths.
- The longest running "Gold Standard" audit in the world. First Report covered 1952-54
- Triennial report published by DOH looking into all maternal deaths in UK
- Changed title from “Why Mothers Die” to “Saving Mothers’ Lives”.
- All maternal deaths: 14 per 100000 maternities (no statistically significant change).
- Direct maternal mortality: slight rise (not statistically significant).
Causes of death:
- Direct: deaths of women while pregnant or within 42 days of termination of pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not accidental or incidental causes.
- Indirect: deaths resulting from previous existing disease, or disease that developed during pregnancy and which was not due to direct obstetric causes, but which was aggravated by the physiological effects of pregnancy.
- Late: deaths occurring between 42 days and one year after the end of pregnancy
Risk Factors contributing to maternal death
(Essentially the same as the lack of decline of maternal mortality)
- Lack of preconception care i.e counselling & support especially for serious physical/mental comorbidities, obesity, assisted reproduction/fertility, and identification of vulnerable/high risk mothers.
- Lack of access to antenatal care
- Migrants (poorer overall health, no medical review, genital mutilation)
- Increasing age of mothers
- Increasing incidence of obese mothers
- Increasing incidence of comorbidities e.g. DM/CVS disease
- Poor lifestyle e.g. smoking/drinking/drugs
Commonest direct causes of maternal death
1) Thromboembolism (again)
=2) Pre-eclampsia/sepsis
4) Amniotic fluid embolism
=5) Haemorrhage/early pregnancy
- Increased numbers of: pre-eclampsia, genital tract sepsis/trauma + inexplicable rise in amniotic fluid embolism.
- Decreased haemorrhage/early pregnancy/ectopic.
- Nil of above: statistically significant.
Commonest indirect cause of maternal death
- Cardiac disease (less healthy diets, smoking, alcohol and the growing epidemic of obesity).
Anaesthetics
- 150 cases reviewed: direct or indirect cause of death also having anaesthetic
Direct anaesthetic deaths:
- 6 deaths – (4.5%) 0.28 per 100000 maternities. Same as previous triennium.
- All but one: Caucasian.
- 4/6: obese (2 were morbidly obese: BMI > 35)
Cases
1) Post-op bronchospasm & resp failure: obese asthmatic lady – failed reintubation during recovery post laparascopic surgery for ectopic pregnancy. Irreversible cardiac arrest.
2) Obese lady, early pregnancy, trainee anaesthetist. High-dose opiate given prior to extubation. In recovery developed respiratory difficulties. Inadequate ventilation, bradycardia, cardiac arrest.
3) Morbidly obese asthmatic lady, elective LSCS, spinal anaesthesia. Post-op agitation and SOB. Fatal cardiac arrest on post-op ward with inadequate resuscitation equipment.
4) Low-dose infusion epidural during labour & forceps delivery. PPH + IVI + syntocinon infusions. Grand mal convulsion + VF arrest – unable to resuscitate. Given 150mls 0.1% bupivacaine IV.
5) Lady with pectus excavatum in mid-pregnancy: â foetal movements, fulminant PET, & HELLP. Hypertensive, hyperreflexic, oliguric, & abnormal LFTs – given labetalol, Mg, & hydralazine. For urgent LSCS: RIJ cannulation unsuccessful but subclavian cannulation successful on the second attempt. Cardiac arrest shortly afterwards – large right haemothorax.
6) Obese woman with longstanding renal problems requiring nephrectomy. Had premature labour and delivery. A few weeks later, she was admitted with fever, loin pain, and ileofemoral venous thrombosis. Planned for drainage of septic focus from remaining kidney under U/S guidance. Pt refused LA and suffered an irreversible cardiac arrest during GA.
Indirect Anaesthetic Deaths
-Further 31 cases where poor perioperative anaesthetic management may have contributed to outcome
- Failure to recognise serious illness
- Poor management of haemorrhage (including syntocinon use): Less than optimum anaesthetic management contributed to many of the 17 maternal deaths from haemorrhage (12 died from PPH).
- Sepsis: Poor anaesthetic management/resuscitation was thought to have contributed to 10 maternal deaths from sepsis (usually failure to appreciate seriousness of maternal condition).
- Pre-eclampsia/eclampsia: 4 women died in relation to poor anaesthetic management (usually related to poor control of systolic blood pressure at time of LSCS/post-operatively)
- Management of obese pregnant women
- Quality of in-house hospital Trust enquiries into serious untoward incidents including maternal deaths: some reports of internal hospital enquiries sent to CEMACH were lacking in insight, improperly conducted, did not include clinicians from relevant specialties, or included clinicians involved directly with the maternal death (potential bias).
Thursday, 3 July 2008
More Reading Material
Previous SAQ papers can be downloaded from the RCOA website here.
AnaesthesiaUK has many many past questions divided into various sections from here and here.
I have grouped all the questions according to SAQ, Long Cases, Short Cases, and Basic Sciences.
I would also look at the CEACCP supplements from 2007-8 that come with the BJA every other month. These topical subjects are excellent SAQ/SOE fodder. If you haven't got hard copies, they can be downloaded here, although you will need to sign in with your BJA subscription details.
The Bulletins from the RCOA can also be a useful source of information, again these can be downloaded from here.
Review articles from the BJA provide exam material too, using archives from 2007 and 2008.
Similarly, review articles from Anaesthesia, using archives from 2007 and 2008. Again, you will need membership details to access these.
Hope this provides some needed direction; there's still more to come!!
AnaesthesiaUK has many many past questions divided into various sections from here and here.
I have grouped all the questions according to SAQ, Long Cases, Short Cases, and Basic Sciences.
I would also look at the CEACCP supplements from 2007-8 that come with the BJA every other month. These topical subjects are excellent SAQ/SOE fodder. If you haven't got hard copies, they can be downloaded here, although you will need to sign in with your BJA subscription details.
The Bulletins from the RCOA can also be a useful source of information, again these can be downloaded from here.
Review articles from the BJA provide exam material too, using archives from 2007 and 2008.
Similarly, review articles from Anaesthesia, using archives from 2007 and 2008. Again, you will need membership details to access these.
Hope this provides some needed direction; there's still more to come!!
Wednesday, 2 July 2008
Buy a library
There are certain essential materials in my opinion which are invaluable for this exam:
Download a copy of the syllabus and use this to break your revision up into topics
Order a copy of the new guide to the FRCA Final Examination. As with the Primary version, this has examples of questions from all sections of the exam. The MCQ section is particularly useful as it is taken from the actual college bank and some do appear in the exam.
Opinion is divided as to whether to use a large textbook or not e.g. Aitkenhead, Pinnock, Hutton etc. This is a personal opinion and one which can be decided by previous experience for Primary and browsing before trying. Candidates will need to purchase/borrow some specialist text-books - many can be ordered from AnaesthesiaUK here or from Amazon. Here is a list I found useful:
General
"Companion to Clinical Anaesthesia Exams (FRCA Study Guides)"Charlie Corke
"Clinical Notes for the FRCA (FRCA Study Guides)"Charles Deakin
MCQ
"Final FRCA: Multiple Choice Questions (FRCA Study Guides)"Michael D. Brunner
"QBase Anaesthesia: MCQs for the Final FRCA v. 5"Edward Hammond
"MCQs for the Final FRCA"Khaled Elfituri
"MCQ's in Anaesthesia (FRCA Study Guides)"A. Ganado
"QBase Anaesthesia: MCQs for the Anaesthesia Final FRCA v. 2 (QBase)"Mark Blunt
"FRCA: MCQs for the Final FRCA: Saunders Self Assessment Series: MCQs for the Final FRCA (FRCA Study Guides)"Karen Henderson
"Practice MCQ's for the Final FRCA (FRCA Study Guides)"Jon Hardman
SAQ
"Anaesthesia & Critical Care" Chris Dodds & Neil Soni
"Short Answer Questions and MCQs in Anaesthesia and Intensive Care"Peter Murphy
"Short Answer Questions in Anaesthesia"Simon Bricker;
"Final F.R.C.A.: Short Answer Questions"J. Nickells
SOE
"The Anaesthesia Science Viva Book" Simon Bricker
"The Clinical Anaesthesia Viva Book"Simon J. Mills
Of course, the A to Z comes in handy too.
Download a copy of the syllabus and use this to break your revision up into topics
Order a copy of the new guide to the FRCA Final Examination. As with the Primary version, this has examples of questions from all sections of the exam. The MCQ section is particularly useful as it is taken from the actual college bank and some do appear in the exam.
Opinion is divided as to whether to use a large textbook or not e.g. Aitkenhead, Pinnock, Hutton etc. This is a personal opinion and one which can be decided by previous experience for Primary and browsing before trying. Candidates will need to purchase/borrow some specialist text-books - many can be ordered from AnaesthesiaUK here or from Amazon. Here is a list I found useful:
General
"Companion to Clinical Anaesthesia Exams (FRCA Study Guides)"Charlie Corke
"Clinical Notes for the FRCA (FRCA Study Guides)"Charles Deakin
MCQ
"Final FRCA: Multiple Choice Questions (FRCA Study Guides)"Michael D. Brunner
"QBase Anaesthesia: MCQs for the Final FRCA v. 5"Edward Hammond
"MCQs for the Final FRCA"Khaled Elfituri
"MCQ's in Anaesthesia (FRCA Study Guides)"A. Ganado
"QBase Anaesthesia: MCQs for the Anaesthesia Final FRCA v. 2 (QBase)"Mark Blunt
"FRCA: MCQs for the Final FRCA: Saunders Self Assessment Series: MCQs for the Final FRCA (FRCA Study Guides)"Karen Henderson
"Practice MCQ's for the Final FRCA (FRCA Study Guides)"Jon Hardman
SAQ
"Anaesthesia & Critical Care" Chris Dodds & Neil Soni
"Short Answer Questions and MCQs in Anaesthesia and Intensive Care"Peter Murphy
"Short Answer Questions in Anaesthesia"Simon Bricker;
"Final F.R.C.A.: Short Answer Questions"J. Nickells
SOE
"The Anaesthesia Science Viva Book" Simon Bricker
"The Clinical Anaesthesia Viva Book"Simon J. Mills
Of course, the A to Z comes in handy too.
Let's have a date
OK, there is just under four months until the MCQ/SAQ paper which is on Tuesday 21st October. Hopefully people have started to revise by now, the big decision of whether to take the exam comes shortly as the opening date for entry is this Friday 4th July. We have until Tuesday 9th September to get the application (& money!) in - probably best not leave until the Monday!
Quite importantly, the paper is set on Tuesday 16th September, meaning that any topical subjects generally for the SAQ and SOE are fair game in journals up to September 2008. I will highlight these as we get nearer the time.
Quite importantly, the paper is set on Tuesday 16th September, meaning that any topical subjects generally for the SAQ and SOE are fair game in journals up to September 2008. I will highlight these as we get nearer the time.
Tuesday, 1 July 2008
A New Beginning
Congratulations to everyone who passed the exam last week - it was no mean feat at all! Unfortunately, I was not successful for a number of reasons; I got a 1+ in the MCQ section which left me on a handicap going into the vivas. I got 2's in the SAQ and Clinical Viva, but had a major hiccup in the Science Viva - I got asked about the intercostal nerve etc and started off OK but then completely blanked. It spiralled downwards from there unfortunately. I thought I had rescued it in pharmacology, talking about conscious sedation & drugs etc, physiology was OK on oxygen delivery, but I appeared to struggle on physics and the Venturi effect of all things. It was a good example of letting an earlier bad section get to me. In hindsight, I should have done more MCQs!! It has been one of the toughest weeks of my career so far, but thanks to some great girlfriend/family/friend/work colleague support, I'm doing OK.
I decided that, despite having been an extremely public humiliation via this blog's reasonably wide stretching and advertising on AnaesthesiaUK, I would carry on blogging. Firstly, I hope it will give heart to others who weren't successfull this time, that they aren't alone in suffering; and secondly, because I know the information I have shared on this blog has helped people - and I hope to continue to do the same for the next batch of people.
You can read my previous efforts in their entirety at an alternative blogsite (I will transfer some relevant stuff from there): http://didntpassthefinal.blogspot.com.
For more excellent advice on how to pass this exam by someone who did pass, visit Exam Intelligence
I decided that, despite having been an extremely public humiliation via this blog's reasonably wide stretching and advertising on AnaesthesiaUK, I would carry on blogging. Firstly, I hope it will give heart to others who weren't successfull this time, that they aren't alone in suffering; and secondly, because I know the information I have shared on this blog has helped people - and I hope to continue to do the same for the next batch of people.
You can read my previous efforts in their entirety at an alternative blogsite (I will transfer some relevant stuff from there): http://didntpassthefinal.blogspot.com.
For more excellent advice on how to pass this exam by someone who did pass, visit Exam Intelligence
Subscribe to:
Comments (Atom)

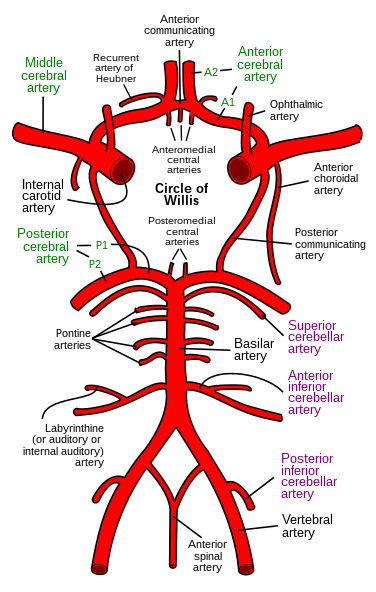{kind=link}
{kind=link}
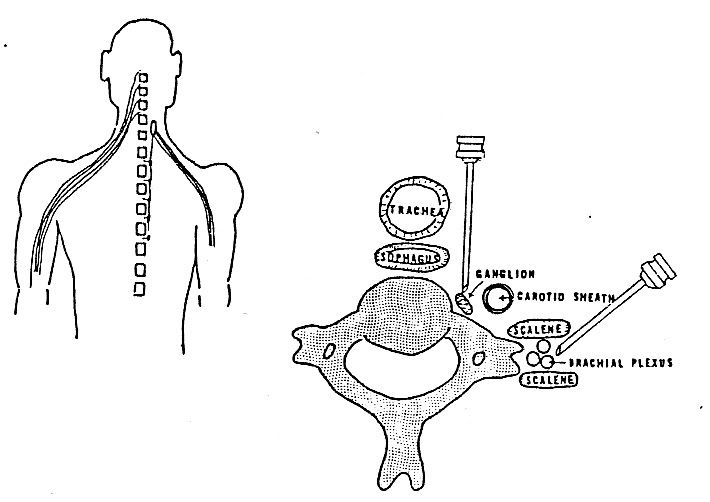{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}